Can Peptides Turn Down the Fire? What the Science Says About Peptides for Inflammation Reduction
Andrew founded Renew Health to change how cardiovascular disease is detected and treated.
Inflammation isn't just something that happens when you sprain your ankle. It's a slow, silent process unfolding in millions of people's arteries right now — and most of them have no idea.
Here's the uncomfortable truth: you can have normal cholesterol, a clean bill of health from your last physical, and still be carrying a hidden fire in your cardiovascular system. That fire — chronic, low-grade inflammation — is one of the primary drivers of heart attacks, stroke, and accelerated aging. And for a growing number of patients, peptide therapy is emerging as a targeted tool to help put it out.
This isn't fringe medicine. It's where cardiovascular science is heading.
Why Does Standard Care Miss the Fire?
Most people equate inflammation with redness and swelling — an acute response that resolves in days. But chronic systemic inflammation is different. It operates below the threshold of obvious symptoms, quietly damaging arterial walls, promoting plaque formation, and destabilizing the kind of deposits most likely to rupture and cause a heart attack.
The inflammatory marker most commonly measured is high-sensitivity C-reactive protein (hs-CRP), produced by the liver in response to immune activation throughout the body. A landmark meta-analysis of 160,309 people across 54 prospective studies found that elevated CRP independently predicted coronary heart disease, ischemic stroke, and vascular mortality — even after adjusting for traditional risk factors like cholesterol and blood pressure. For every threefold increase in CRP concentration, coronary heart disease risk climbed by 37%. (Emerging Risk Factors Collaboration, 2010, The Lancet)
The same cholesterol numbers that look fine on paper can coexist with dangerous arterial inflammation. This is precisely why Renew's approach goes beyond the standard lipid panel.
Where Do Peptides Enter the Picture?
Peptides are short chains of amino acids — the molecular building blocks your body already uses to run virtually every biological process. Unlike broad-spectrum anti-inflammatory drugs (which suppress the immune system globally), certain peptides can modulate inflammation through highly targeted mechanisms: dialing down specific cytokines, protecting endothelial tissue, and supporting the body's own healing pathways.
Think of them as precision messengers that speak your cells' own language.
The research is still evolving, but several peptides show genuine promise for reducing systemic inflammation — particularly in the context of cardiovascular protection.
What Does the Science Say? Key Peptides and What They Do
1. BPC-157: A Locally Derived Anti-Inflammatory Agent
BPC-157 (Body Protection Compound-157) is a 15-amino-acid peptide derived from a protective protein naturally found in gastric juice. It's been studied extensively in preclinical models for its cytoprotective, anti-inflammatory, and tissue-repair properties.
In one study examining BPC-157's effect on periodontal inflammation, rats treated with BPC-157 showed significantly reduced plasma extravasation (a marker of vascular inflammation), decreased histological signs of inflammation, and reduced alveolar bone resorption compared to controls — all without altering normal blood circulation in healthy tissue. (Keremi et al., 2009, Journal of Physiology and Pharmacology)
This selective action is key: BPC-157 appears to reduce pathological inflammation without broadly suppressing immune function. In preclinical models across multiple organ systems — gut, tendon, cardiac tissue, nervous system — it has consistently demonstrated anti-inflammatory effects alongside a notably clean safety profile.
A 2025 systematic review of BPC-157 in orthopedic sports medicine confirmed that the peptide "reduces inflammatory cytokines" and "enhances several pathways involved in cell growth and angiogenesis" — with no adverse effects observed in preclinical safety studies. (Emerging Use of BPC-157, PMC12313605)
Important caveat: Most BPC-157 research is still preclinical. We don't yet have large-scale human RCTs. At Renew, we apply this data carefully and within appropriate clinical context.
2. Thymosin Beta-4: Endothelial Protection and Immune Regulation
Thymosin beta-4 (Tβ4) is a naturally occurring peptide involved in actin regulation, cell migration, and wound healing — but its anti-inflammatory effects are gaining increasing attention.
In cardiac tissue, Tβ4 has been shown to promote post-injury repair while modulating the inflammatory response: supporting angiogenesis (new blood vessel growth), reducing scar tissue formation, and shifting immune cell behavior toward regeneration rather than continued inflammation. In post-myocardial infarction animal models, Tβ4-treated subjects showed significantly better outcomes — including less inflammation, fewer deaths from cardiac rupture, and improved heart function.
For patients with established cardiovascular disease, this regenerative-anti-inflammatory axis is especially relevant.
3. GLP-1 Receptor Agonists: Metabolic Inflammation at the Source
The GLP-1 receptor agonists — Ozempic, Wegovy, Mounjaro — have dominated public conversation around weight loss. But their anti-inflammatory effects on the cardiovascular system go far deeper than metabolism.
GLP-1 agonists appear to protect the endothelium directly, reduce oxidative stress, and shift macrophage behavior away from the pro-inflammatory (M1) phenotype that accelerates plaque development. In the LEADER trial, liraglutide reduced major adverse cardiovascular events by 13% in high-risk patients — not primarily through LDL reduction, but through pathways that include endothelial protection and inflammation modulation.
For patients at Renew who are already on a GLP-1 medication, this is one of the reasons we view it as more than a weight loss drug.
Does Targeting Inflammation Directly Actually Work?
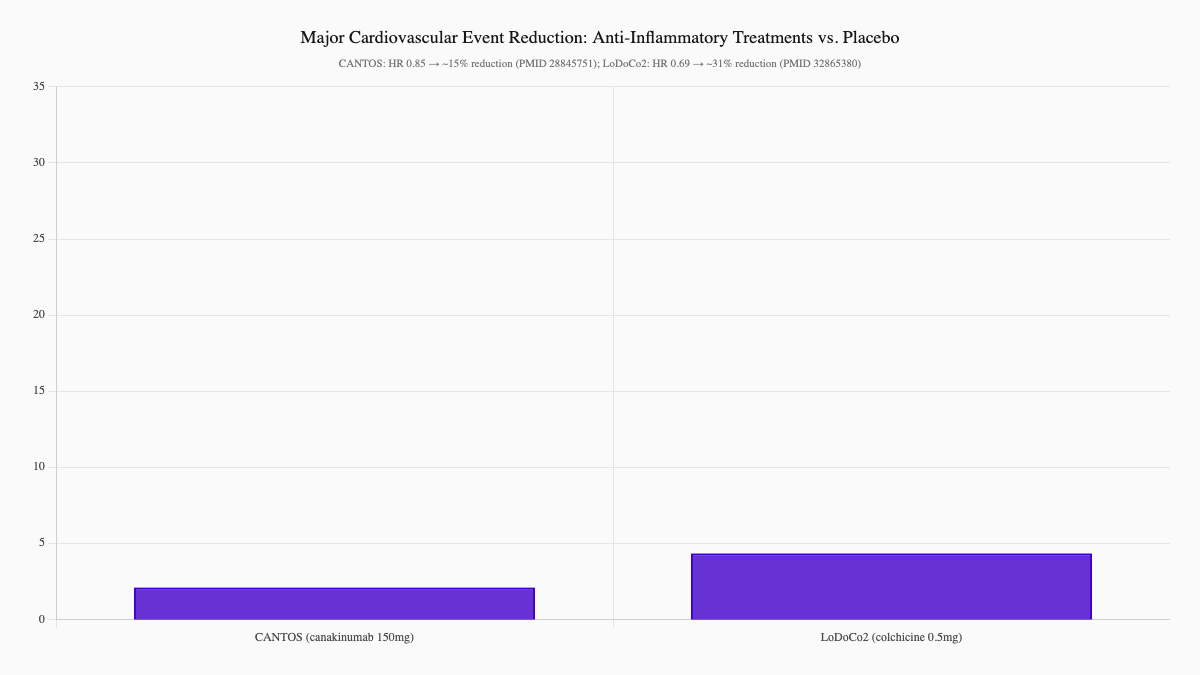
The most compelling evidence that inflammation is a direct driver of cardiovascular events — not just a bystander — comes from two landmark clinical trials.
The CANTOS trial tested canakinumab, a biologic that specifically targets interleukin-1β (IL-1β), a key inflammatory cytokine. In patients with prior heart attacks and elevated CRP, canakinumab reduced cardiovascular events significantly — without meaningfully changing LDL cholesterol. The protection came entirely from inflammation reduction. (Ridker et al., 2017, The New England Journal of Medicine)
The LoDoCo2 trial tested low-dose colchicine — an anti-inflammatory drug used for gout — in patients with stable coronary disease. It reduced major cardiovascular events by 31% compared to placebo. Again, not through cholesterol. Through inflammation. (Fiolet et al., 2020, The New England Journal of Medicine)
These trials didn't study peptides specifically. But they proved the principle: targeting inflammation directly prevents heart attacks. Peptides that reduce systemic inflammation through similar cytokine pathways operate on exactly this premise.
David's Story: What Happened When We Looked Deeper?
David was 54 when he first came to Renew. By every conventional measure, he was in decent shape — nonsmoker, moderate exercise, cholesterol "within normal limits." His GP had told him to keep doing what he was doing.
But David had fatigue that wouldn't lift. Joint aches that moved around. A family history of heart disease he couldn't stop thinking about.
We ran a comprehensive panel. His hs-CRP was 4.8 mg/L — well above the optimal threshold of 1.0 mg/L. His Lp-PLA2 was elevated, indicating active vascular inflammation. His CIMT scan showed early carotid wall thickening — not yet a crisis, but a signal his arteries were aging faster than his calendar age.
We identified two root causes: undiagnosed insulin resistance and a gut inflammation pattern that was driving systemic immune activation.
David started a protocol that included dietary changes targeting insulin resistance, gut support with BPC-157, omega-3 fatty acids at therapeutic doses, and vitamin D optimization. We tracked his inflammatory markers every 12 weeks.
By month six, his hs-CRP had dropped to 1.4 mg/L. Lp-PLA2 normalized. His energy returned — something he'd quietly stopped expecting. His follow-up CIMT showed no progression.
"I thought I was just getting older," he told us. "Turns out my body was sending signals I didn't know how to read."
What Are the Warning Signs That Inflammation May Be Active?
Chronic inflammation rarely announces itself dramatically. But these patterns should prompt deeper investigation:
- Persistent fatigue — especially unrelated to sleep quality or exertion
- Joint aches that migrate or come without obvious injury
- Brain fog or difficulty with sustained concentration
- Elevated hs-CRP (above 1.0 mg/L; above 3.0 is high risk)
- Metabolic syndrome — central obesity, high triglycerides, low HDL, high fasting glucose
- Family history of early heart disease (first-degree relative before age 65)
- Insulin resistance or prediabetes — often undiagnosed on standard panels
- Sleep apnea — a major but underdiagnosed driver of vascular inflammation
If any of these apply to you, standard cholesterol testing is not enough.
How Does Renew Find the Fire and Trace It to Its Source?
At Renew, inflammation isn't an abstract concern — it's something we measure directly, track over time, and treat at the root.
Our inflammation assessment includes:
-
CIMT ultrasound — Direct imaging of carotid artery wall thickness, detecting atherosclerosis before it calcifies or shows on a calcium score. This is the most sensitive early-warning tool we have for arterial inflammation. Learn more about CIMT
-
Advanced inflammatory biomarkers — hs-CRP, Lp-PLA2, myeloperoxidase (MPO), fibrinogen, and uric acid. Together, these give us a multi-angle picture of immune activity in and around your arterial walls.
-
Root cause testing — Insulin sensitivity, fasting insulin, HbA1c, gut permeability markers, vitamin D status, and sleep assessment. We can't put out the fire if we don't know what's fueling it.
-
Serial tracking — We retest at intervals. Inflammation responds to treatment; we want to see your markers move.
What Works? An Evidence-Tiered Framework
We don't recommend peptides in isolation. They work best as part of a protocol that addresses the full inflammatory picture.
Foundation: Lifestyle Modifications
- Mediterranean-style diet — the PREDIMED trial showed a 30% reduction in major cardiovascular events vs. a low-fat control diet
- Zone 2 aerobic exercise — lowers inflammatory cytokines, improves insulin sensitivity, supports mitochondrial health
- Sleep optimization — 7–9 hours of quality sleep; treat sleep apnea if present
- Stress management — chronic cortisol elevation directly fuels inflammatory signaling
Targeted Supplements
- Omega-3 fatty acids (EPA/DHA) — reduce TNF-α, IL-6, and CRP; stabilize plaque
- Vitamin D — deficiency is independently associated with elevated CRP and cardiovascular risk; optimize to 50–80 ng/mL
- Magnesium — supports endothelial function and reduces vascular reactivity
- CoQ10 — especially important for patients on statins
Peptide Protocols (When Clinically Appropriate)
- BPC-157 — for gut-driven systemic inflammation and tissue-level repair
- Thymosin Beta-4 — for post-injury recovery and endothelial support
- GLP-1 agonists — for patients with metabolic inflammation at the root of their cardiovascular risk
Pharmacologic (When Indicated)
- Low-dose colchicine — now with strong RCT evidence for cardiovascular event reduction in stable coronary disease
- Statins — beyond LDL lowering, they independently reduce hs-CRP
- Low-dose aspirin — for select high-risk patients in consultation with their cardiologist
What Are the Important Considerations for Peptide Therapy?
Peptide therapy is not a magic lever. There are real considerations to discuss with your provider:
Delivery: Most therapeutic peptides cannot be taken orally — they're broken down in the digestive tract before reaching circulation. Subcutaneous injection is the standard route. Most patients adapt quickly.
Regulatory status: BPC-157 and Thymosin Beta-4 are not FDA-approved for any indication. They are used off-label by clinicians who have reviewed the preclinical evidence and determined appropriate use for individual patients.
Oncology screening: Because some peptides promote growth-related pathways (angiogenesis, cell proliferation), we screen carefully before starting any protocol. Patients with active cancer or unknown masses require additional evaluation.
Individual variation: Not every peptide works equally well for every patient. We personalize protocols based on your inflammatory markers, root cause findings, and treatment response.
What Can You Do Now?
If you've been told your labs are "fine" but something still feels off — or if you have risk factors that standard care hasn't fully addressed — here's how to start:
-
Ask for inflammatory biomarkers. Request hs-CRP, Lp-PLA2, and a fasting insulin level at your next visit. Don't settle for a cholesterol panel as the final word on your cardiovascular risk.
-
Consider a CIMT scan. It's 15 minutes, no radiation, no contrast, and it shows you directly what's happening inside your arterial walls. It's one of the most informative preventive tests available. Learn more →
-
Come in for a comprehensive evaluation. We'll review your history, your current markers, and help you understand whether peptide therapy — or any of the other tools in our protocol — makes sense for your situation.
Ready to Take a Closer Look at What's Driving Your Inflammation?
Chronic inflammation is measurable, trackable, and — with the right approach — reversible. At Renew, we use advanced imaging, comprehensive biomarker panels, and evidence-informed protocols to find the fire and put it out before it does serious damage.
Whether you're starting from scratch or looking to optimize an existing prevention plan, we're here to help you build a strategy that goes beyond standard care.
View our services and pricing →
Learn about CIMT cardiovascular imaging →
References
-
Emerging Risk Factors Collaboration. (2010). C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: an individual participant meta-analysis. The Lancet, 375(9709), 132–140. PMID 20031199
-
Ridker PM, et al. (2017). Antiinflammatory therapy with canakinumab for atherosclerotic disease. The New England Journal of Medicine, 377(12), 1119–1131. PMID 28845751
-
Fiolet ATL, et al. (2020). Colchicine in patients with chronic coronary disease. The New England Journal of Medicine, 383(19), 1838–1847. PMID 32865380
-
Keremi B, et al. (2009). Antiinflammatory effect of BPC 157 on experimental periodontitis in rats. Journal of Physiology and Pharmacology, 60 Suppl 7, 115–22. PMID 20388954
This article is for educational purposes only and does not constitute medical advice. Peptide therapies discussed here are not FDA-approved for the indications described. Always consult with a qualified healthcare provider before beginning any new treatment protocol.
Related Reading:
Ready to see your actual risk?
Advanced metabolic testing, arterial imaging, and a personalized prevention plan — built around your numbers.
View Memberships