Heart Health Myths Debunked: What the Latest Science Really Says
Andrew founded Renew Health to change how cardiovascular disease is detected and treated.
Most people believe they would know if something were wrong with their heart. Tracy believed the same thing.
At 52, she was the picture of health — regular exercise, clean diet, healthy weight, no smoking. When she felt pressure in her chest and pain between her shoulder blades during arm exercises, she chalked it up to soreness from a recent rotator cuff surgery. She went home for the holidays. On Christmas Day, she felt what she described as an electric shock in her wrist and jaw. Her family rushed her to the emergency department. Cardiac catheterization revealed blockages in four arteries. She was in immediate danger and didn't know it.
Tracy's story isn't unusual. What's unusual is that she made it in time.
Heart health myths — the kind that sound reasonable, even scientific — keep people from getting screened, treated, or even taking their symptoms seriously. This article breaks down the most dangerous ones, and what the latest evidence actually says.
Myth 1: Is Heart Disease Really Just a Man's Problem?
This is one of the most persistent and deadly misconceptions in medicine.
Heart disease is the leading cause of death for both men and women in the United States. Since 1984, more women than men have died from cardiovascular disease each year. Yet women are still less likely to be screened aggressively and more likely to dismiss their own symptoms — in part because the cultural image of a "heart attack victim" is still a middle-aged man clutching his chest.
Women's symptoms often look different. Jaw pain, back pain, fatigue, nausea — these are common presentations in women that get dismissed or attributed to stress, anxiety, or muscle soreness. Just like Tracy.
Plaque buildup also starts earlier than most people realize. Fatty deposits can begin forming in arteries during childhood and adolescence. By the time someone reaches their twenties, the process may already be underway.
If you're a woman — or if you love one — don't assume heart disease isn't your concern.
Myth 2: Is High Blood Pressure Just Part of Getting Older?
Blood pressure does tend to rise with age as arteries stiffen — but that doesn't mean it should be accepted or left untreated.
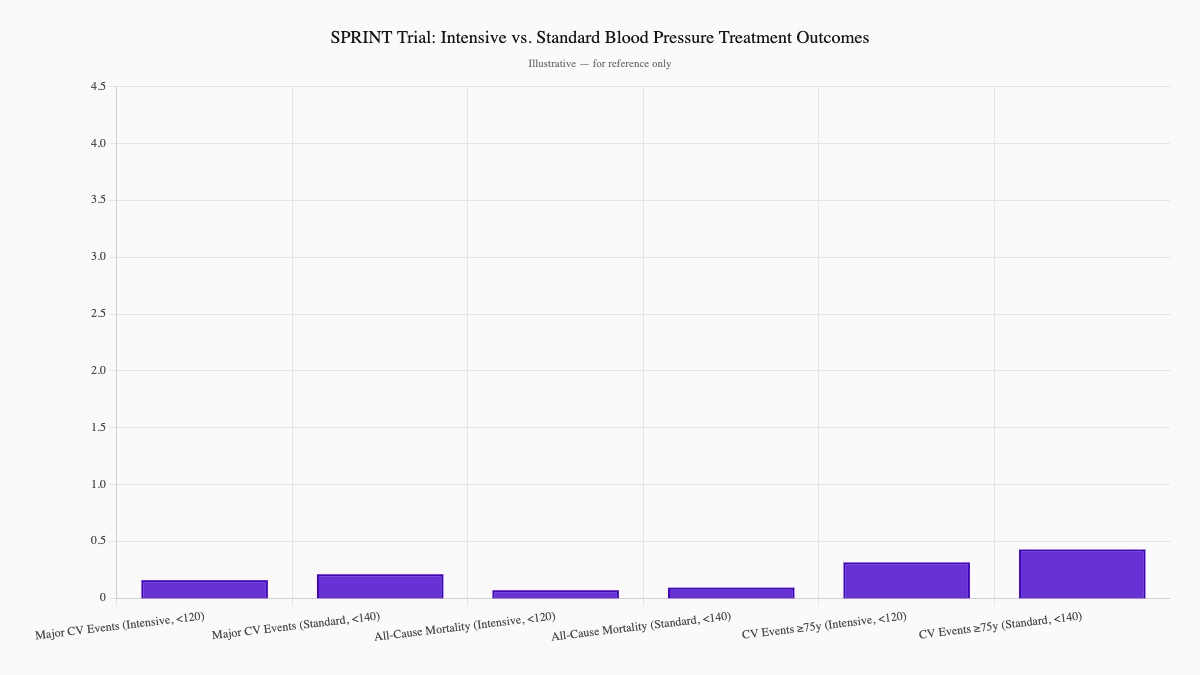
The SPRINT trial (Systolic Blood Pressure Intervention Trial) tested this directly. Older adults treated to a systolic blood pressure below 120 mmHg had significantly fewer heart attacks, strokes, and deaths compared to those treated to the standard target of below 140 mmHg. The benefit held even in adults over 75. (Supiano et al., 2017, Journal of the American Geriatrics Society)
The longstanding concern was that aggressive treatment would cause falls or dizziness in older patients. SPRINT addressed that directly — and while side effects require monitoring, the cardiovascular benefit was real and substantial.
Current guidelines reflect this: most adults, regardless of age, should aim to keep blood pressure below 130/80 mmHg. For most people, that requires a combination of lifestyle changes and medication.
Accepting high blood pressure as a normal part of aging isn't being realistic. It's leaving a major risk factor unmanaged.
Myth 3: Won't You Know When Something's Wrong With Your Heart?
No, you won't. Not reliably.
High blood pressure is called the "silent killer" because it almost never produces symptoms — even at dangerously elevated levels. Heart disease itself can develop over decades without a single warning sign. The first symptom of coronary artery disease is a heart attack in roughly 50% of cases.
The only way to know your numbers is through regular testing: blood pressure checks, comprehensive lipid panels, and — for those at elevated risk — imaging that looks directly at your arteries.
This is exactly why advanced tools like CIMT (Carotid Intima-Media Thickness) imaging matter. CIMT uses ultrasound to directly measure the thickness of arterial walls, revealing plaque buildup before it causes a blockage or a cardiac event. It's painless, takes about 15 minutes, and provides information that no standard blood test can.
Tracy didn't skip her checkups. She just didn't have access to the right tests. Don't assume a normal annual physical means you're in the clear.
Learn what CIMT can reveal about your arterial health →
Myth 4: Does Heart Failure Mean the Heart Has Stopped?
These two terms get conflated constantly, and the confusion carries real risk.
Cardiac arrest is when the heart suddenly stops beating. Without CPR or defibrillation within minutes, it is fatal. Heart failure is a chronic condition in which the heart continues to beat, but doesn't pump as effectively as it should.
Heart failure develops gradually, often over years, and is highly treatable. Many people with heart failure live active, full lives with the right medications, lifestyle adjustments, and monitoring. The key is catching it and managing it — which starts with understanding what it actually is.
| Feature | Heart Failure | Cardiac Arrest |
|---|---|---|
| Onset | Gradual, chronic | Sudden, acute |
| Heart still beating? | Yes, but weakly | No |
| Symptoms | Shortness of breath, swelling, fatigue | Collapse, no pulse, no consciousness |
| Emergency? | Requires ongoing management | Always immediately life-threatening |
| Treatment | Medication, lifestyle, monitoring | CPR, defibrillation |
If you're told you have "early heart failure" or "reduced ejection fraction," that is not a death sentence. It is a signal to act.
Myth 5: If Heart Disease Runs in Your Family, Can You Change Anything?
Genetics load the gun. Lifestyle pulls the trigger — or doesn't.
Yes, a family history of early heart disease significantly raises your risk. But parents don't just pass down genes. They also pass down habits: eating patterns, activity levels, stress responses. Separating genetic risk from lifestyle-driven risk is harder than most people realize.
What the research makes clear: lifestyle changes make a substantial difference even in people with high genetic risk. Regular exercise, a diet rich in vegetables and whole grains, maintaining a healthy weight, and managing blood pressure and cholesterol can dramatically reduce cardiovascular events — even in those with familial hypercholesterolemia or a strong family history.
Genetics tells us where to pay extra attention. It doesn't tell us the outcome is fixed.
Myth 6: Is Exercise Dangerous After a Heart Event?
This myth keeps recovering patients sedentary — and makes outcomes worse.
The evidence is consistent: exercise is one of the most powerful tools in cardiac recovery. A comprehensive meta-analysis of 85 randomized controlled trials found that exercise-based cardiac rehabilitation reduces cardiovascular mortality, recurrent cardiac events, and hospitalizations while improving quality of life and exercise capacity. (Dibben et al., 2023, European Heart Journal)
The key word is structured. Supervised cardiac rehab programs tailor activity to each patient's condition. They're safe. They're effective. And patients who complete them live longer.
For stable heart disease, the recommendation is at least 150 minutes of moderate activity per week. Sitting still is not protecting your heart — it's weakening it.
If you've had a heart event and you're avoiding all physical activity out of fear, talk to your provider about a supervised cardiac rehab program.
Myth 7: Can Supplements Replace Medication and Lifestyle?
This is where wishful thinking collides with the data.
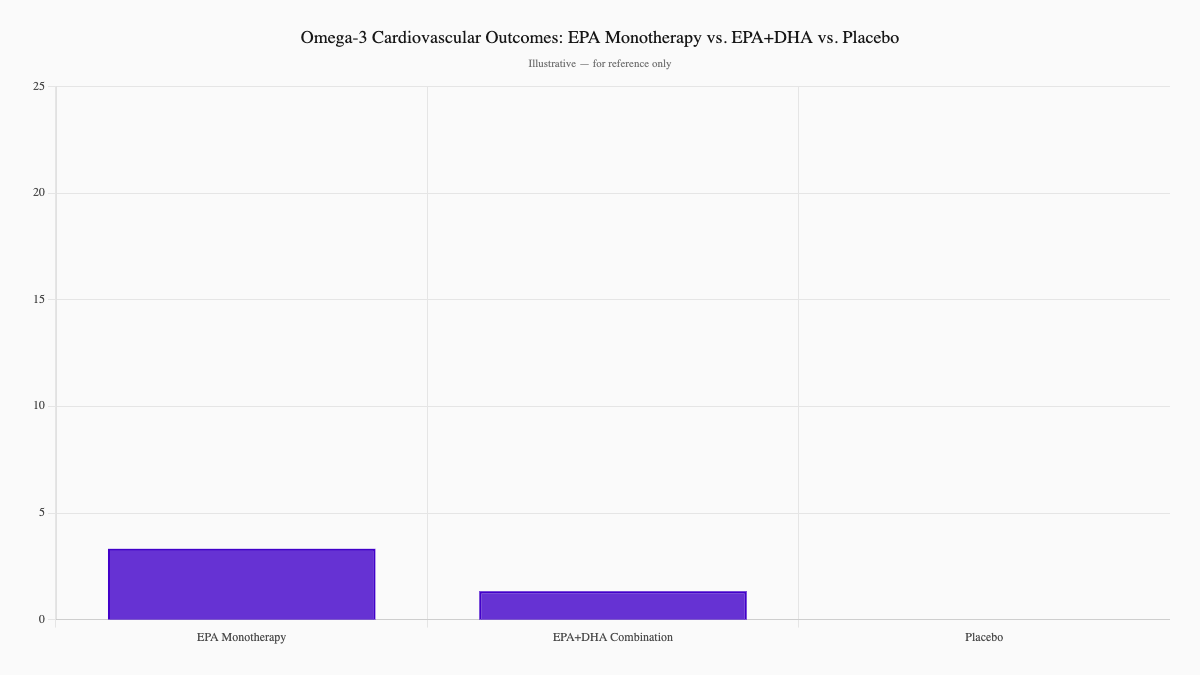
Fish oil supplements have been heavily marketed as cardiovascular protection. The reality is more complicated. A large meta-analysis of 38 randomized controlled trials found that omega-3 fatty acids overall reduced cardiovascular mortality and some non-fatal cardiac events — but the benefit was driven primarily by high-dose EPA monotherapy, not the EPA+DHA combination found in standard over-the-counter fish oil. EPA+DHA showed only modest, inconsistent benefits across outcomes. (Bernasconi et al., 2021, eClinicalMedicine)
The bottom line: high-dose prescription EPA (icosapentaenoic acid, as studied in REDUCE-IT) has demonstrated meaningful benefit in high-risk patients — but that's a very different product, dose, and population than the fish oil capsules at a pharmacy.
Other common supplement myths:
- Vitamins E, C, and beta-carotene were widely believed to prevent heart disease due to antioxidant effects. Multiple large clinical trials showed no cardiovascular benefit.
- Coconut oil and butter are often marketed as "heart-healthy fats." Both are high in saturated fat, which raises LDL cholesterol and increases cardiovascular risk.
Statins, by contrast, have decades of robust trial data behind them. They work. They reduce risk. They're not a sign of failure — they're a tool that saves lives when diet and exercise alone aren't enough.
Medications work best alongside lifestyle changes, not instead of them. But supplements are not a substitute for either.
Myth 8: Does Quitting Smoking After Years Still Help?
Some of the most powerful data in preventive medicine is on smoking cessation — and none of it supports giving up on quitting.
A Cochrane systematic review found moderate-certainty evidence that smoking cessation reduces CVD death, non-fatal heart attacks, and non-fatal strokes in patients with established cardiovascular disease. (Wu et al., 2022, Cochrane Database of Systematic Reviews)
The timeline of recovery after quitting is striking:
- 20 minutes: Heart rate and blood pressure begin to drop
- 12 hours: Carbon monoxide levels in the blood return to normal
- 1 year: Risk of heart attack is cut roughly in half compared to continuing smokers
- 10 years: Risk of dying from heart disease approaches that of a lifelong non-smoker
Even if you've smoked for 30 or 40 years, the body begins to repair itself. The damage already done doesn't disappear — but it stops accumulating, and the cardiovascular system responds.
Quitting is the single most impactful thing a smoker can do for their heart. It's never too late.
Myth 9: Do Popular "Healthy" Foods Actually Protect Your Heart?
A few specific food myths deserve direct attention.
Butter and coconut oil as "healthy fats": Both are high in saturated fat, which raises LDL cholesterol more than it raises HDL. This increases the risk of plaque buildup and cardiovascular events. The marketing around these foods outpaces the evidence.
Pink Himalayan salt as a healthier alternative: It contains trace minerals, but in amounts far too small to make a clinical difference. What matters is sodium content — which is essentially the same in all salt types. Excess sodium raises blood pressure and strains the cardiovascular system.
Dark chocolate and red wine as heart protectors: Both contain antioxidants and polyphenols, but the concentrations in typical commercial products are too low to produce meaningful cardiovascular benefit. For alcohol specifically, any potential benefit from light drinking is offset by elevated blood pressure and other harms at higher intake levels.
The better framework: Don't focus on adding or eliminating single foods. Focus on overall dietary patterns — more vegetables, whole grains, lean proteins, and unsaturated fats; less processed food, added sugar, and excess sodium. The pattern matters more than any single food.
How Does Renew Test for What Standard Care Misses?
Standard care checks blood pressure and runs a basic cholesterol panel. That's a start — but it often misses what's actually happening inside your arteries.
At Renew, we go further:
CIMT Imaging: A quick, painless ultrasound that directly measures arterial wall thickness and identifies early plaque. It tells us what's actually happening in your arteries — not just what your bloodwork suggests.
Advanced Lipid Testing: Standard panels measure total LDL. We measure LDL particle number and size, lipoprotein(a), and apolipoprotein B — markers that significantly change the risk picture for many patients.
Comprehensive Cardiovascular Risk Assessment: We evaluate your full risk profile — family history, biomarkers, imaging — and build a prevention strategy tailored to where you are now.
If you've been told your numbers look fine but something doesn't feel right — or if you have a family history of heart disease and want to know your actual arterial status — CIMT is one of the most informative tests you can do.
Learn more about CIMT imaging at Renew →
What Does Tracy's Story Really Mean?
Tracy exercised. She ate well. She didn't smoke. She had no obvious risk factors — and still had blockages in four arteries on Christmas Day.
The lesson isn't that prevention is futile. It's that traditional risk markers aren't the full picture, and assuming you'd know if something were wrong is one of the most dangerous assumptions you can make.
Cardiac disease is mostly silent until it isn't. The window to intervene — before a heart attack, before permanent damage — requires proactive testing. Not waiting for symptoms. Not assuming a normal physical means you're clear.
Your Next Steps
- Get your numbers. Blood pressure, full lipid panel, fasting glucose — at minimum.
- Consider CIMT imaging. Especially if you have a family history, are over 45, or have any modifiable risk factors.
- Don't wait for symptoms. The absence of symptoms is not the same as the absence of disease.
- If you smoke, quit. Even after years, the benefit of stopping is real and measurable.
- Exercise intentionally. 150 minutes of moderate activity per week is a therapeutic dose, not just a lifestyle preference.
The myths about heart health aren't harmless. They delay action at exactly the moment when action matters most.
Ready to Know Your Real Risk?
Renew offers comprehensive cardiovascular risk assessment — including CIMT imaging and advanced lipid testing — to help you understand what's actually happening in your arteries, not just what your standard bloodwork shows.
See our services and pricing →
Schedule a free consultation to build a personalized cardiovascular prevention plan.
Sources
-
Supiano MA, et al. (2017). Applying the Systolic Blood Pressure Intervention Trial Results to Older Adults. Journal of the American Geriatrics Society, 65(1), 16–21. https://pubmed.ncbi.nlm.nih.gov/28111758/
-
Bernasconi AA, Wiest MM, Lavie CJ, Milani RV, Laukkanen JA. (2021). Effect of omega-3 fatty acids on cardiovascular outcomes: A systematic review and meta-analysis. eClinicalMedicine, 41, 101159. https://pubmed.ncbi.nlm.nih.gov/34505026/ [Overall omega-3 reduced CV mortality and non-fatal MI; EPA monotherapy showed stronger effects than EPA+DHA]
-
Dibben G, Faulkner J, Oldridge N, et al. (2023). Exercise-based cardiac rehabilitation for coronary heart disease: a meta-analysis. European Heart Journal, 44(6), 452–469. https://pubmed.ncbi.nlm.nih.gov/36746187/
-
Wu AD, Lindson N, Hartmann-Boyce J, et al. (2022). Smoking cessation for secondary prevention of cardiovascular disease. Cochrane Database of Systematic Reviews, 8, CD014936. https://pubmed.ncbi.nlm.nih.gov/35938889/
Ready to see your actual risk?
Advanced metabolic testing, arterial imaging, and a personalized prevention plan — built around your numbers.
View Memberships