Heart Disease in Women: The Silent Threat That's Hiding in Plain Sight
Andrew founded Renew Health to change how cardiovascular disease is detected and treated.
Here's something that might surprise you: heart disease kills more women than breast cancer—yet most women I meet still think of it as a "man's problem."
I get it. When we picture a heart attack, we imagine someone clutching their chest, sweating, gasping—the classic movie moment. But that picture is based almost entirely on how men experience heart disease. Women's hearts tell a different story, and it's one we're way too often missing.
Why Is Heart Disease So Deadly for Women—and Why Doesn't Anyone Talk About It?
Heart disease is the leading cause of death in women in the US. Over 60 million women are living with some form of it, and in 2023 alone, it claimed nearly 305,000 lives—one in every five female deaths.
So why does it still feel like a secret?
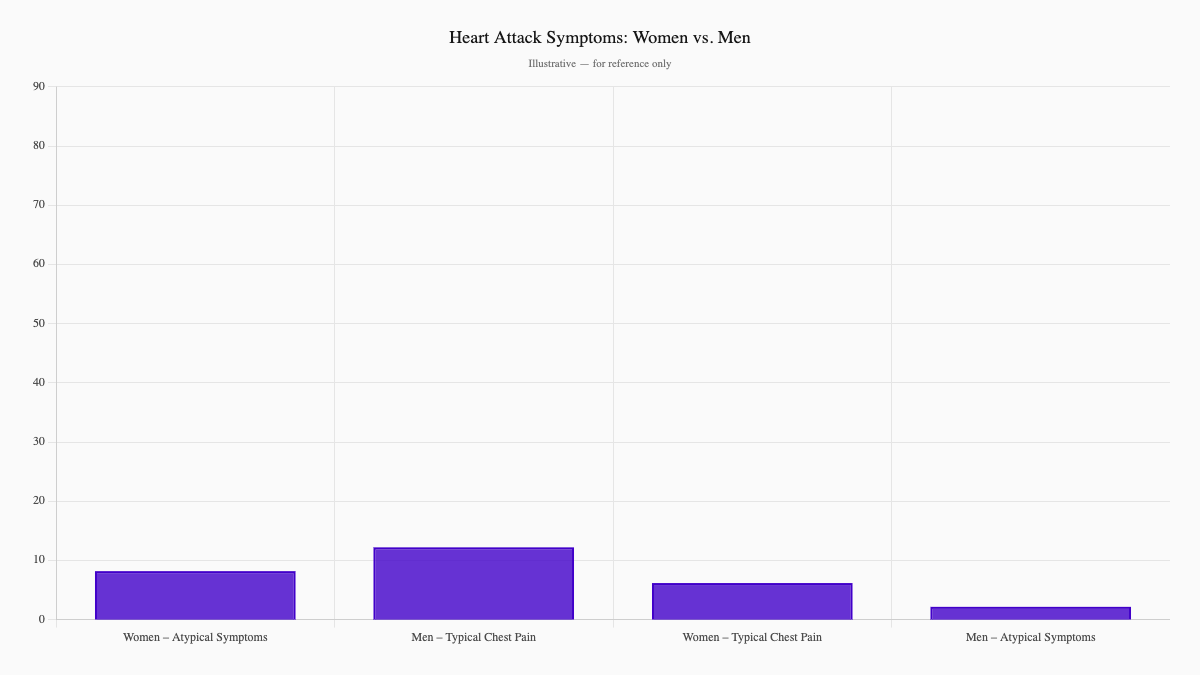
Because women's symptoms don't fit the textbook. While men typically present with crushing chest pain, women often experience something entirely different—subtle signals that get dismissed as indigestion, stress, or just "being tired."
Research shows that women presenting with myocardial infarction are significantly more likely than men to experience atypical symptoms—nausea, fatigue, shortness of breath, back or jaw pain—and less likely to report classic chest pain at all. That's not a small gap. It's a massive blind spot in how we diagnose what's killing us.¹
Why Does Standard Cardiac Care Miss Women?
Here's where things get frustrating. There are conditions that specifically target women, yet they fly under the radar of conventional cardiology.
INOCA (Ischemia with No Obstructive Coronary Arteries)—Women can have classic heart attack symptoms—crushing chest pain, even elevated troponin levels—yet their angiogram comes back "normal." The problem isn't blocked arteries; it's that the tiny blood vessels, the microvasculature, aren't working right. Women are disproportionately affected by this condition, yet it took far too long for the medical community to take it seriously.²
SCAD (Spontaneous Coronary Artery Dissection)—A tear in the artery wall that can happen suddenly, especially in women under 50. It often strikes during pregnancy or after emotional stress, and it's now recognized as a leading cause of heart attacks in young women. It is also frequently misdiagnosed.³
The research backs this up. Women are less likely to be diagnosed promptly, less likely to receive aggressive treatment, and more likely to have worse outcomes—not because their hearts are more fragile, but because we've been applying a male template to a female problem.
What Happened to Megan?
Let me tell you about a patient we'll call Megan.
Megan was 42, a mother of two, and genuinely healthy by every standard measure. She didn't smoke. Her cholesterol was fine. She exercised regularly. One afternoon while playing with her toddler at the park, she felt mild chest discomfort and shortness of breath. She figured it was indigestion—maybe she was just tired.
Two days later, the discomfort still hadn't gone away. She saw her primary care doctor, who told her it was probably stress and anxiety.
Three days after that, Megan collapsed at home.
Emergency services diagnosed a massive heart attack. Cardiac catheterization revealed SCAD—a spontaneous tear in her left anterior descending artery. She needed emergency stenting and spent a week in the ICU.
Megan had zero traditional risk factors. Her standard cardiac workup would have labeled her "low risk." And yet, she nearly died.
This is the reality for thousands of women. Their hearts are asking for help in a language we've never bothered to learn.
What Do Heart Attacks Actually Look Like in Women?
Here's what women's heart attacks actually look like:
- Indigestion or burning in the chest
- Pain in the back, neck, jaw, or arms
- Shortness of breath without exertion
- Unusual fatigue that won't quit
- Nausea or vomiting
- Lightheadedness
- A vague sense that something is off
Notice anything? None of these scream "heart attack" to most people. That's exactly why they're so dangerous.
If you're a woman experiencing any of these—especially if they're new, unexplained, or won't resolve—get it checked. Push for more testing if something feels wrong. Trust your gut. It's probably nothing, but "probably nothing" is not a risk worth taking with your heart.
How Does Renew Find What Other Providers Miss?
At Renew, we don't wait for a classic presentation. We look deeper, using tools designed to catch heart disease in women before it becomes a crisis.
Coronary Artery Calcium (CAC) Scoring
Standard risk calculators often underestimate women's risk because they weren't built with female physiology in mind. CAC scoring detects the plaque that's silently building up—even when you feel perfectly fine. This matters especially for women whose "normal" cholesterol numbers may be hiding real trouble.
Sex-Specific Troponin Thresholds
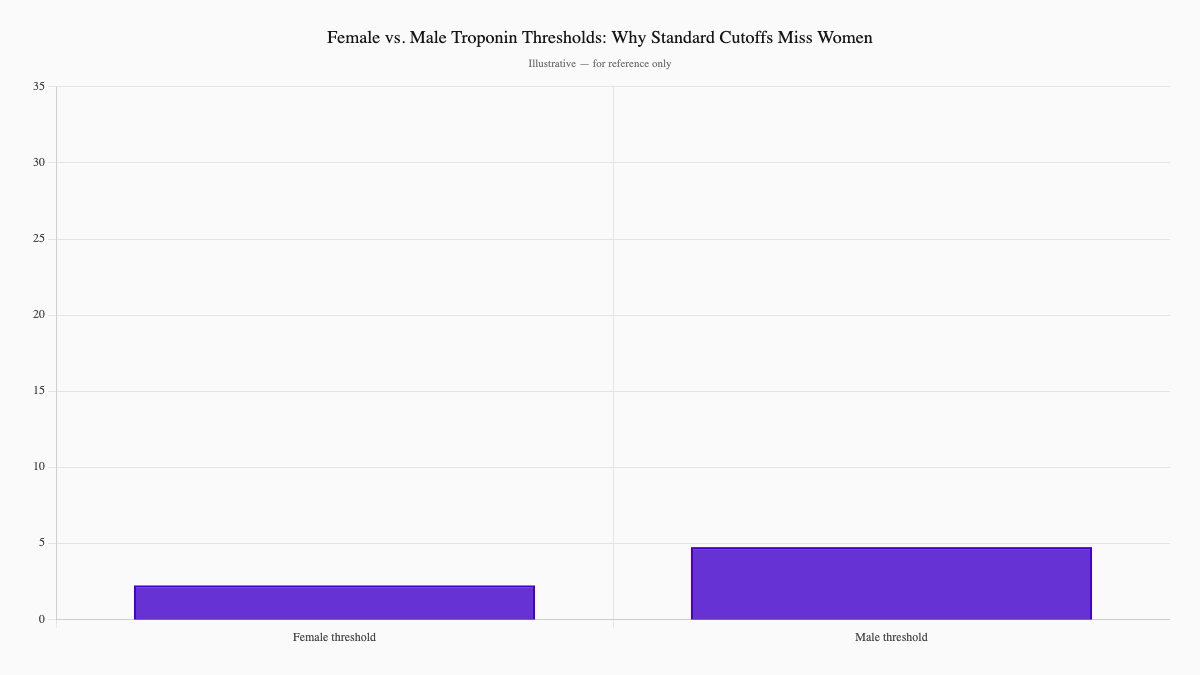
Here's something most doctors don't know: women have lower troponin levels at baseline than men. The standard "normal" cutoff was derived from male data—and when you apply it to women, you miss real heart injury.
A 2024 systematic review found that more than 90% of high-sensitivity troponin assays show lower female-specific thresholds—approximately 16 ng/L for women versus 34 ng/L for men. Using male cutoffs in women leads directly to underdiagnosis.⁴
When we apply female-specific thresholds, we detect significantly more heart attacks in women. That's not a marginal improvement. That's lives saved.
Looking at the Root Cause
We also look beyond the usual suspects. Conditions that disproportionately affect women—polycystic ovary syndrome, hypertensive disorders of pregnancy, premature menopause, autoimmune inflammatory conditions—raise cardiovascular risk meaningfully. We factor these in because they're part of your real risk profile, not some arbitrary formula.
To understand your vascular age and catch early arterial disease, consider a CIMT scan—a carotid intima-media thickness test that gives us a direct window into your vascular health before symptoms ever begin.
What Treatments Actually Work for Women?
The good news? When we find it, we can treat it effectively.
Intensive statin therapy works for women. In the PROVE IT-TIMI 22 trial, women on high-dose atorvastatin achieved a 42.8% reduction in LDL cholesterol within 30 days—dropping to a median of 60 mg/dL—with a 25% relative reduction in major cardiovascular events compared to standard dosing. Women benefited at least as much as men, with no additional safety concerns.
Beyond statins, we address the full picture: inflammation (through markers like hsCRP), endothelial function, and metabolic health. We don't just lower numbers. We protect the entire cardiovascular system.
What Can You Do Right Now?
If you're a woman over 40—or younger with risk factors—here's your action plan:
-
Know your numbers beyond the basics. Ask for CAC scoring. Request advanced lipid testing (particle number, Lp(a)). These reveal what standard cholesterol panels miss.
-
Track your risk factors. Pregnancy complications? Early menopause? PCOS? Autoimmune conditions? These aren't just "women's health issues"—they are cardiovascular risk factors.
-
Don't accept "you're fine." If something feels wrong, push for more testing. You know your body better than anyone.
-
Consider a CIMT scan. Carotid intima-media thickness testing gives us a window into your vascular health—one of the most powerful early-detection tools we have. Learn more about CIMT scanning at Renew.
What's the Bottom Line?
Heart disease in women isn't rare, mysterious, or "atypical." It's common, it's deadly, and it's been hiding in plain sight because we built our understanding on male bodies.
But here's what gives me hope: when we look for it with the right tools, we find it. And when we find it, we can treat it.
Megan survived. She's now an advocate for women's heart health. But she shouldn't have had to nearly die to get the answers she deserved.
You shouldn't have to either.
Ready to take a closer look at your heart health? Our team uses advanced, sex-specific diagnostics to find what standard workups miss. View our pricing and packages →
Or start with a CIMT scan—a non-invasive test that reveals your true vascular age in under an hour.
References
-
Schulte KJ, Mayrovitz HN. Myocardial Infarction Signs and Symptoms: Females vs. Males. Cureus. 2023 Apr 13;15(4):e37522. PMID: 37193476
-
Noel Bairey Merz C, et al. Treatment of coronary microvascular dysfunction. Cardiovasc Res. 2020. PMID: 32087007
-
Zeven K. Pregnancy-Associated Spontaneous Coronary Artery Dissection in Women: A Literature Review. Curr Ther Res Clin Exp. 2023. PMID: 36993873
-
Cao M, et al. Systematic Review of Sex-specific High Sensitivity Cardiac Troponin I and T Thresholds. Clin Ther. 2024 Dec. PMID: 39505672
This article is for educational purposes only and does not constitute medical advice. Always consult with your healthcare provider for personalized guidance.
Ready to see your actual risk?
Advanced metabolic testing, arterial imaging, and a personalized prevention plan — built around your numbers.
View Memberships