Heart Attack and Stroke Risk After 50: What You Need to Know
Andrew founded Renew Health to change how cardiovascular disease is detected and treated.
Here's something most people don't realize: You can feel completely fine, have no obvious symptoms, and still be walking toward a heart attack. That's exactly what happened to Mike.
At age 50, Mike was walking out of the cafeteria at work with his morning coffee when he felt a sudden pain in the center of his chest. He assumed it was heartburn and kept walking. He stopped at a friend's desk to chat and got very lightheaded. His friend told him he looked gray and offered to call emergency services. Mike declined.
He drove himself home. His wife—a former heart cath tech—insisted on driving him to urgent care. As soon as they put an EKG on him, they told him he was having a heart attack and called an ambulance. He had a 90% occlusion in his right coronary artery and received a stent.
The kicker? Mike wasn't overweight. He'd had no previous symptoms. But his high cholesterol had been ignored by his primary care provider for years. The heart attack struck without warning.
This is the uncomfortable truth about cardiovascular risk after 50: it sneaks up on you.
Why Does Cardiovascular Risk Climb After 50?
Once you hit your 50s, the math changes. Conditions like hypertension, high cholesterol, diabetes, and obesity become more common—and each one adds extra strain on your heart and blood vessels.
The danger grows when these risks pile up together. High blood pressure alone explains over a quarter of heart disease cases. Add high cholesterol, diabetes, or excess weight, and your chance of a major event increases significantly.
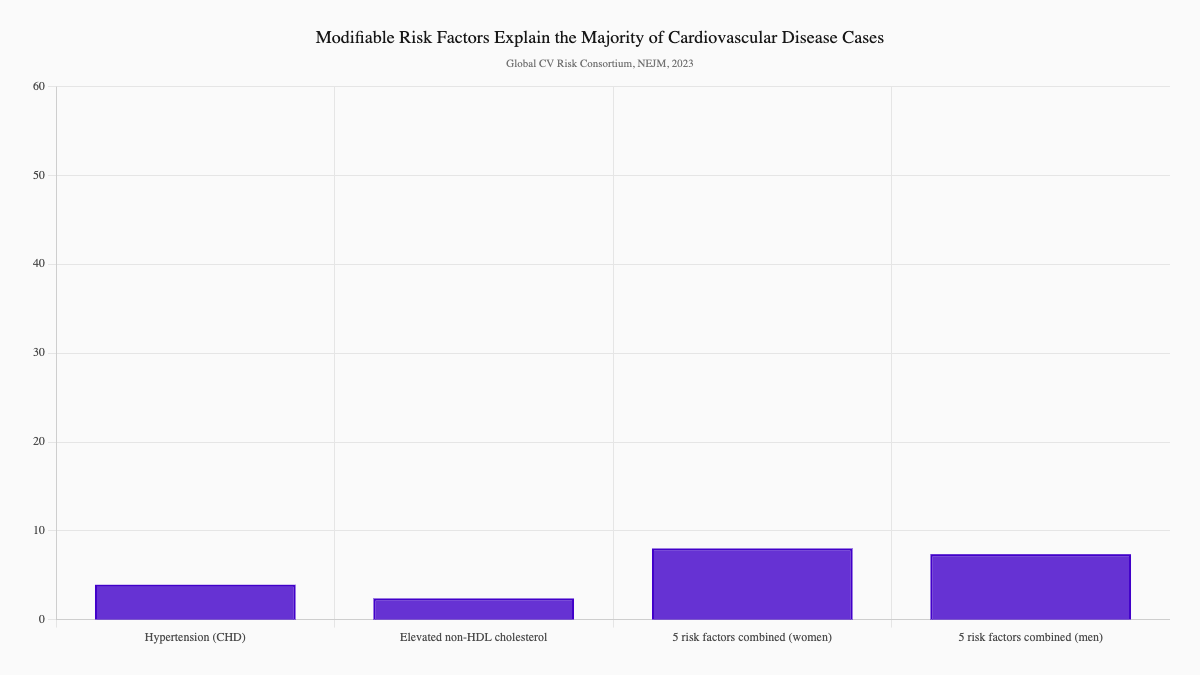
Here's what the research shows: five modifiable risk factors—hypertension, high cholesterol, diabetes, obesity, and smoking—explain more than half of all cardiovascular disease cases worldwide (Global Cardiovascular Risk Consortium, 2023, NEJM). That's not a small contribution. That's the majority of risk coming from things you can actually change.
What Does the Science Tell Us About the Strongest Risks?
High Blood Pressure and Cholesterol Are King
Blood pressure and cholesterol remain the two biggest players in heart attack and stroke risk. A large global meta-analysis found that systolic blood pressure of 130 mmHg or higher explained 28% of coronary heart disease cases. Elevated non-HDL cholesterol of 130 mg/dL or more explained another 17% (Global Cardiovascular Risk Consortium, 2023, NEJM).
Together, those two factors account for nearly half of the burden.
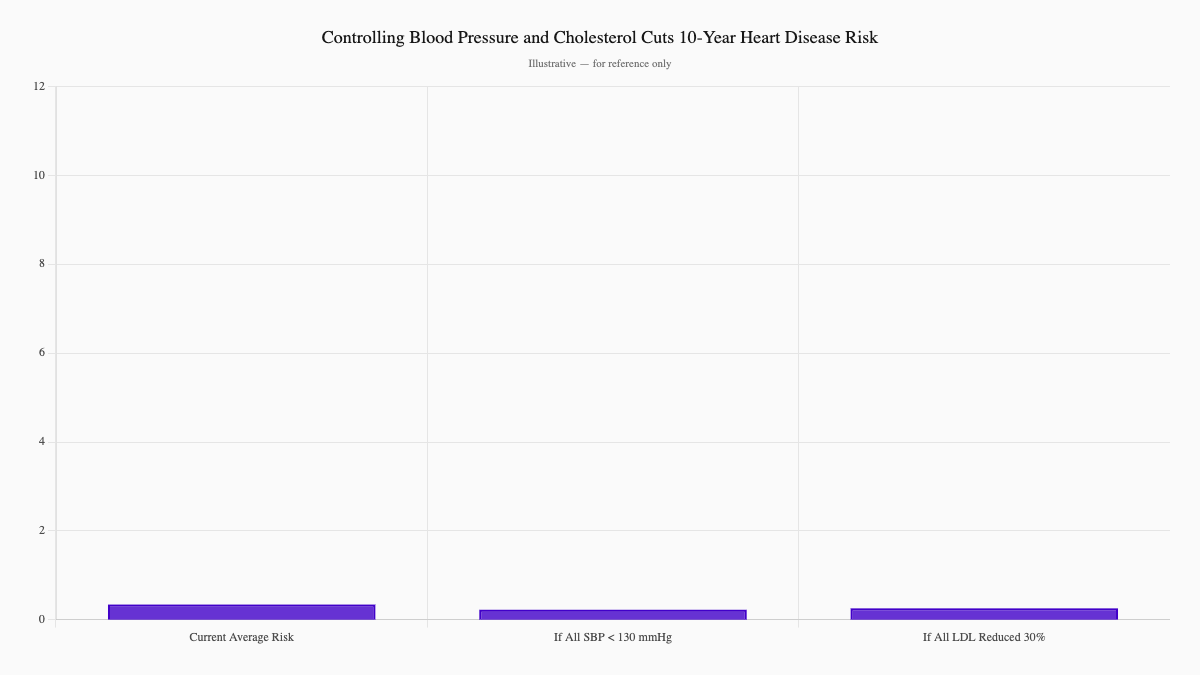
But here's the hopeful part: the same research showed that control makes a measurable difference. If everyone lowered blood pressure below 130 mmHg, the average 10-year heart disease risk would fall from 10.7% to 7.0%. If LDL cholesterol dropped by 30%, that same risk would fall to 8.0%.
That's not theoretical. That's measurable protection.
Diabetes Adds Serious Fuel
Diabetes is a powerful independent risk factor. According to the same Global Cardiovascular Risk Consortium analysis, diabetes was one of the five key modifiable risk factors explaining over half of incident cardiovascular disease cases worldwide (Global Cardiovascular Risk Consortium, 2023, NEJM). Chronically elevated blood sugar damages blood vessels and accelerates atherosclerosis—the plaque buildup that leads to heart attacks.
The Weight Connection
Higher body mass index (BMI) also contributes meaningfully to cardiovascular risk. When combined with blood pressure, cholesterol, smoking, and diabetes, BMI formed a cluster that explained 57.2% of cardiovascular disease cases among women and 52.6% among men (Global Cardiovascular Risk Consortium, 2023, NEJM).
Carrying extra weight adds pressure on your heart and blood vessels. When layered on top of other risks like smoking or high blood pressure, the effects multiply.
Which Lifestyle Risks Hit Harder Than You'd Think?
Smoking: No Safe Level
This one stings because many people assume cutting down is good enough. It's not.
A meta-analysis of 141 cohort studies covering 55 million people found that smoking just one cigarette per day raises the risk of coronary heart disease by 48% in men and 57% in women (Hackshaw et al., 2018, BMJ). For stroke, even one cigarette a day increases risk by 25% in men and 31% in women.
The conclusion was unambiguous: no safe level of smoking exists. Cutting down helps, but only quitting fully lowers the risk significantly.
Physical Inactivity Is Quietly Deadly
Physical inactivity tends to get overlooked—it doesn't feel as dangerous as smoking. But the numbers tell a different story.
An analysis of 196 studies covering more than 30 million people found that adults who met the recommended 150 minutes per week of moderate activity had a 31% lower risk of dying from any cause compared to inactive adults, and a 29% lower risk of dying from cardiovascular disease (Garcia et al., 2023, British Journal of Sports Medicine). Even small increases in activity among the least active adults provided the strongest gains. If everyone reached this activity level, nearly 16% of premature deaths could be avoided.
Alcohol: The J-Curve
Alcohol shows a complicated pattern. A meta-analysis of 27 prospective studies covering more than 1.4 million individuals found that low alcohol intake was associated with a 15% lower risk of total stroke and a 19% lower risk of ischemic stroke. However, heavy drinking flipped the outcome—increasing the risk of total stroke by 20% (Zhang et al., 2014, International Journal of Cardiology).
This J-shaped relationship means moderation matters. Light intake may offer some benefit, but once drinking becomes heavy, the damage to blood vessels and blood pressure outweighs any protection.
What Did Mike's Story Teach Us About Silent Risk?
Let's go back to Mike, because his story contains lessons that apply to anyone over 50.
Mike was relatively fit and had no warning signs. He'd never had chest pain, shortness of breath, or any of the classic symptoms people associate with heart attacks. What he did have was high cholesterol that his doctor had been "monitoring" for years without treating.
When he felt chest pain at work, he dismissed it as heartburn. His legs were so weak he had to hold onto the cubicle walls to walk. His wife saved his life by insisting they go to urgent care immediately.
Mike was lucky. He got there in time, received a stent, and has been fine since. He now takes statins to control his cholesterol.
The takeaway: Don't wait for symptoms to take action. Mike had none—and his high cholesterol was silently damaging his arteries for years. By the time you feel something, the damage may already be done.
Which Heart Attack and Stroke Warning Signs Can't You Ignore?
Even when symptoms appear, people often talk themselves out of taking them seriously. Here's what to watch for:
Heart attack warning signs:
- Chest pain or pressure lasting more than a few minutes
- Pain radiating to your arm, jaw, neck, or back
- Shortness of breath
- Cold sweats, nausea, or lightheadedness
Stroke warning signs (think FAST):
- Face drooping
- Arm weakness
- Speech difficulty
- Time to call 911
A "mini-stroke" (transient ischemic attack, or TIA) is a temporary blockage that signals a high risk of a full stroke. Never ignore it.
How Does Renew Approach Cardiovascular Risk Differently?
At Renew, waiting for a heart attack isn't a strategy. We take a proactive, evidence-based approach to understanding your actual cardiovascular risk before something goes wrong.
CIMT Imaging
We use Carotid Intima-Media Thickness (CIMT) ultrasound to look directly at your arteries. This isn't a stress test you pass or fail—it's actual imaging of your arterial wall thickness, which reveals plaque buildup before it causes symptoms.
CIMT is quick, painless, and gives us a baseline that no standard blood work can match. It's one of the most reliable early detection tools for atherosclerosis.
Learn more about CIMT imaging at Renew →
Advanced Lipid Testing
Standard cholesterol panels miss a lot. We go deeper with testing that includes:
- LDL particle number and size
- Lipoprotein(a)—a genetic marker strongly linked to heart disease
- Apolipoprotein B
These tests reveal your actual risk profile, not just what a basic panel shows.
What Actually Works? Evidence-Based Treatments for Cardiovascular Risk
Medications That Protect
Statins are the cornerstone of cholesterol management. For adults aged 40–75 with one or more cardiovascular risk factors and an estimated 10-year CVD risk of 10% or greater, statins provide at least a moderate net benefit (US Preventive Services Task Force, 2022, JAMA).
The benefit extends to older adults as well. A meta-analysis of 29 randomized controlled trials found that LDL-lowering therapy reduced the risk of major vascular events by 26% per 1 mmol/L reduction in LDL cholesterol—and the benefit was equally strong in patients aged 75 and older as in younger patients (Gencer et al., 2020, Lancet).
ACE inhibitors lower blood pressure and reduce strain on the heart, making them the preferred therapy in most patients with hypertension and elevated cardiovascular risk.
Antiplatelet therapy (such as low-dose aspirin) remains central to secondary prevention in patients with established cardiovascular disease, significantly reducing the risk of a repeat event.
Lifestyle: The Foundation
Medications work best when paired with lifestyle changes. The evidence is clear:
- Move more: Reaching 150 minutes of moderate activity weekly is associated with a 31% lower risk of premature death
- Quit smoking: No safe level exists—every cigarette raises your risk
- Limit alcohol: If you drink, keep it light. Heavy drinking reverses any benefit
- Manage stress: Chronic stress contributes to inflammation and cardiovascular damage
What Are Your Action Steps?
Here's where to start:
-
Know your numbers. Schedule a comprehensive cardiovascular assessment that includes CIMT imaging and advanced lipid testing. Don't rely on basic blood work alone.
-
Don't wait for symptoms. Mike felt fine until he wasn't. Plaque builds silently over years.
-
Talk to a provider about your risk. If you're over 50—or have a family history of heart disease—it's time to be proactive.
-
Consider CIMT testing. It's one of the best ways to see your actual arterial health and catch problems before they become emergencies.
What's the Bottom Line on Cardiovascular Risk After 50?
After 50, your risk of heart attack and stroke increases—but it's not fixed. Hypertension, high cholesterol, diabetes, obesity, smoking, and physical inactivity all raise the risk. The good news? Every one of these is modifiable.
Mike assumed he was healthy. His doctor had been "monitoring" his cholesterol for years without treating it. Don't make the same mistake.
Lowering blood pressure, controlling cholesterol, staying active, and quitting smoking create real, measurable impact. Medications like statins add another layer of protection—one that works just as well in older adults as in younger ones.
Taking action on these risks after 50 isn't just prevention—it's an investment in a healthier heart, a stronger brain, and more years of quality life.
Ready to Understand Your Real Cardiovascular Risk?
Don't wait for a wake-up call like Mike's. Renew Health offers comprehensive cardiovascular risk assessment including CIMT imaging and advanced lipid testing.
View pricing and book an appointment →
Schedule a free consultation to discuss your risk factors and build a personalized prevention plan.
Sources
-
Global Cardiovascular Risk Consortium. (2023). Global effect of modifiable risk factors on cardiovascular disease and mortality. New England Journal of Medicine, 389(14), 1273–1285. https://pubmed.ncbi.nlm.nih.gov/37632466/
-
Hackshaw, A., Morris, J. K., Boniface, S., Tang, J.-L., & Milenković, D. (2018). Low cigarette consumption and risk of coronary heart disease and stroke: meta-analysis of 141 cohort studies in 55 study reports. BMJ, 360, j5855. https://pubmed.ncbi.nlm.nih.gov/29367388/
-
Garcia, L., Pearce, M., Abbas, A., et al. (2023). Non-occupational physical activity and risk of cardiovascular disease, cancer and mortality outcomes: a dose-response meta-analysis of large prospective studies. British Journal of Sports Medicine, 57(15), 979–989. https://pubmed.ncbi.nlm.nih.gov/36854652/
-
US Preventive Services Task Force. (2022). Statin use for the primary prevention of cardiovascular disease in adults: US Preventive Services Task Force recommendation statement. JAMA, 328(8), 746–753. https://pubmed.ncbi.nlm.nih.gov/35997723/
-
Gencer, B., Marston, N. A., Im, K., et al. (2020). Efficacy and safety of lowering LDL cholesterol in older patients: a systematic review and meta-analysis of randomised controlled trials. Lancet, 396(10263), 1637–1643. https://pubmed.ncbi.nlm.nih.gov/33186535/
-
Zhang, C., Qin, Y. Y., Chen, Q., et al. (2014). Alcohol intake and risk of stroke: a dose-response meta-analysis of prospective studies. International Journal of Cardiology, 174(3), 669–677. https://pubmed.ncbi.nlm.nih.gov/24820756/
Ready to see your actual risk?
Advanced metabolic testing, arterial imaging, and a personalized prevention plan — built around your numbers.
View Memberships