The Future of Preventive Cardiology: How Technology Is Changing the Game
Andrew founded Renew Health to change how cardiovascular disease is detected and treated.
Heart disease remains the world's leading cause of death—but here's what most people don't realize: up to 80% of heart attacks and strokes are preventable. The problem isn't that we don't know how to prevent heart disease. It's that we've been looking in the wrong places, at the wrong time.
For decades, cardiology focused on treating heart disease after it appeared—bypass surgery, stents, medications. We waited for symptoms. We waited for a heart attack. Then we reacted.
But the future of heart health isn't about reacting. It's about predicting. It's about catching risk decades before it becomes disease.
And that future is already here.
Are We Starting Too Late to Prevent Heart Disease?
The traditional approach to heart disease goes something like this: you turn 40, get your cholesterol checked, and if the numbers look okay, you're told you're "fine." Then you come back in five years.
Here's the issue: by the time standard tests flag a problem, damage may already be happening.
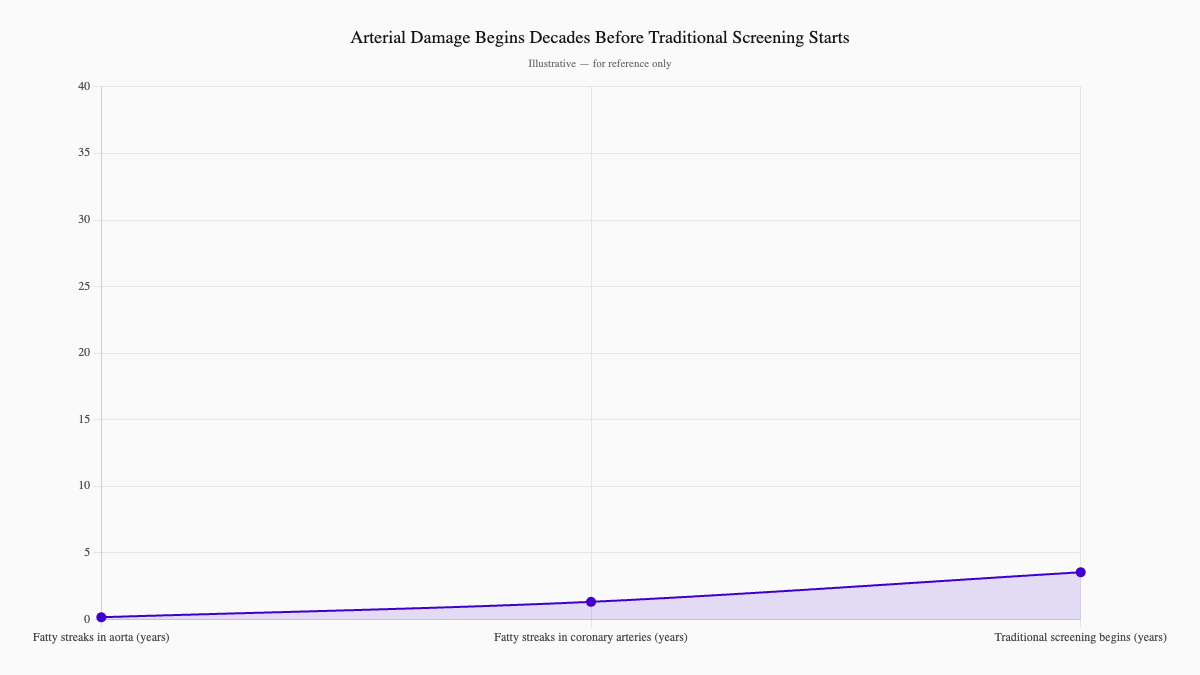
The Bogalusa Heart Study showed that fatty streaks—the earliest signs of atherosclerosis—appear in the aorta of children as young as age 2. By age 15, half of kids already have these streaks in their coronary arteries.
We're treating heart disease like it's an adult problem. But the foundation is laid decades earlier.
This is why the paradigm is shifting—from reactive cardiology to preventive cardiology. From "let's fix it when it breaks" to "let's see it coming and stop it first."
What New Technologies Are Actually Changing Cardiology?
Several technologies are converging to make early detection real. Here's what you need to know:
Wearables: Your Heart, Monitored 24/7
Smartwatches and fitness trackers aren't just counting steps anymore. Modern devices use photoplethysmography (PPG) sensors and single-lead ECG technology to detect irregular heart rhythms—most importantly, atrial fibrillation (AFib).
AFib is tricky because it often has no symptoms. You might feel occasional "flutters" and dismiss them as stress or too much coffee. But AFib significantly increases stroke risk—and many people don't know they have it until it's too late.
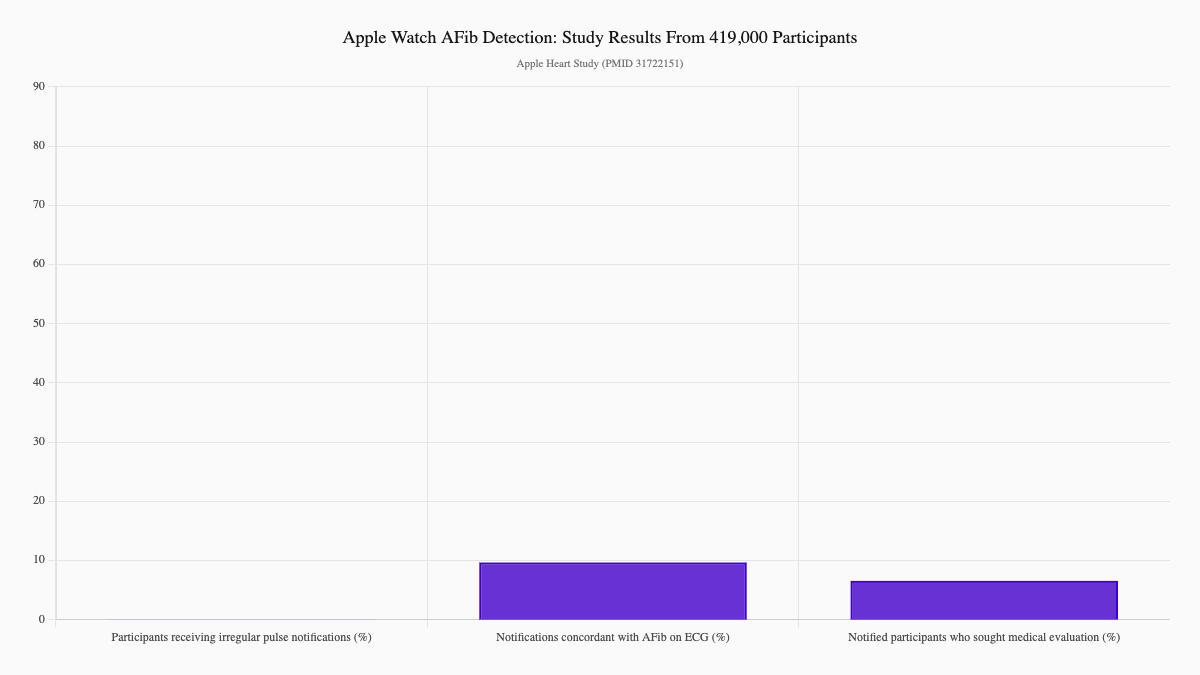
In a massive study of over 419,000 Apple Watch users, 0.52% received notifications about an irregular pulse. Among participants who were notified and wore follow-up ECG patches, 34% had confirmed atrial fibrillation—and the smartwatch notifications had an 84% positive predictive value when cross-referenced against simultaneous ECG readings. Even more telling: 57% of those notified sought medical evaluation on their own. (Perez MV et al., Apple Heart Study, N Engl J Med. 2019;381:1909–1917)
That's the power of continuous monitoring. You're not waiting for an annual checkup. Your device is watching while you sleep, work, and exercise.
AI and Machine Learning: Predicting Risk Before It Happens
Traditional risk calculators like the Framingham Score use a handful of variables—age, cholesterol, blood pressure, smoking status. They're useful, but they miss a lot.
Machine learning changes everything. These models can analyze thousands of variables simultaneously: imaging data, genetic markers, lifestyle factors from wearables, electronic health records. They find patterns that human clinicians might overlook.
A landmark study using data from 378,256 UK primary care patients found that machine-learning algorithms—particularly neural networks—outperformed the standard ACC/AHA risk calculator, correctly identifying 7.6% more patients who went on to develop cardiovascular disease, while reducing unnecessary treatment of others. (Weng SF et al., PLoS One. 2017;12(4):e0174944)
This isn't science fiction. It's happening now.
Genetic Testing: Knowing Your Inherited Risk
You can't change your genes. But knowing what they say can save your life.
Lipoprotein(a), often called Lp(a), is one of the strongest genetic risk factors for heart disease. Unlike cholesterol, which responds to diet and exercise, Lp(a) is largely determined by genetics. High Lp(a) can raise your cardiovascular risk even if your LDL cholesterol is perfectly healthy.
The American Heart Association now recommends that everyone have their Lp(a) checked at least once. Yet most conventional clinics still don't routinely test for it. (Reyes-Soffer G et al., AHA Scientific Statement, Arterioscler Thromb Vasc Biol. 2022;42:e48–e60)
That's a gap we're closing at Renew.
Advanced Imaging: Seeing What Traditional Tests Miss
Standard stress tests and echocardiograms have limitations. They might show that your heart is pumping fine—but miss early signs of damage hiding beneath the surface.
4D Flow MRI is a game-changer. This technology tracks blood flow through the heart and vessels in three dimensions over time. It can detect turbulent flow, abnormal wall shear stress, and vortex patterns that signal early dysfunction—long before symptoms appear. Combined with AI analysis, these imaging techniques are making early detection not just possible, but routine. (Zhuang B et al., Quant Imaging Med Surg. 2021;11(9):4193–4210)
What Was Marcus's Wake-Up Call?
Marcus is a 47-year-old executive. He exercises regularly, maintains a healthy weight, and has no chronic conditions. By all accounts, he's doing everything right.
He also felt occasional "flutters" in his chest but figured they were just work stress. His father had a stroke at 62, but Marcus considered himself healthy.
One Tuesday night, Marcus couldn't sleep. Something felt off. He decided to wear his Apple Watch to bed—something he rarely did.
By Wednesday morning, the watch had flagged three irregular rhythm alerts. His heart rate had spiked to 168 bpm during the night.
When Marcus shared his ECG readings with his Renew physician, we ordered a 48-hour Holter monitor. The results confirmed paroxysmal atrial fibrillation with rapid ventricular response. His echocardiogram showed normal heart function—no structural damage yet.
We started him on apixaban (a blood thinner to reduce stroke risk) and referred him for catheter ablation. Three months later, the procedure was successful. Marcus remains in normal sinus rhythm.
Here's what haunts me about Marcus's case: if he hadn't worn his watch that night, his AFib might have gone undetected for years. Every month without treatment would have been another month of elevated stroke risk.
His story illustrates why we're so passionate about preventive cardiology. We don't want to wait for the heart attack. We want to catch the warning signs first.
What Heart Disease Warning Signs Might You Be Missing?
Heart disease often sneaks up silently. But there are clues if you know where to look:
- Occasional heart palpitations or "flutters" — especially if they come and go
- Unexplained fatigue — more than usual, even with adequate sleep
- Shortness of breath during activities that used to be easy
- Family history of heart disease or stroke (especially early onset — before age 55 in men or 65 in women)
- High Lp(a) — a genetic risk factor that standard cholesterol tests don't catch
- Sleep apnea — linked to higher cardiovascular risk
- Borderline numbers — cholesterol or blood pressure that's "close enough" to not worry about, but trending the wrong direction
The traditional healthcare system often waits until you're "sick enough" to treat. We're different. We look for risk before it becomes disease.
Curious about your vascular age? Learn more about CIMT imaging at Renew.
What Does Renew Do Differently in Preventive Cardiology?
At Renew, we believe in catching risk early—then doing something about it.
Here's how our preventive cardiology program works:
Comprehensive Risk Assessment
We don't rely on a single cholesterol number. Our panels include:
- Advanced lipid testing — including Lp(a), ApoB, and LDL particle number
- Inflammatory markers — hsCRP, which standard panels typically skip
- Metabolic markers — insulin, HbA1c, and fasting glucose
- Genetic testing — for inherited risk factors like Lp(a) variants
CIMT Imaging
Carotid Intima-Media Thickness (CIMT) ultrasound measures the thickness of the walls of your carotid arteries. It's a direct measure of arterial health—essentially a window into what's happening throughout your entire cardiovascular system.
This isn't a test you get only "if you're high risk." It's for anyone who wants to know their true vascular age. Learn more about CIMT imaging →
Continuous Monitoring Integration
If you wear a smartwatch or fitness tracker, we can review your data. Heart rate variability, sleep patterns, activity levels—these all paint a picture of your cardiovascular fitness.
AI-Powered Risk Prediction
We use machine learning models to synthesize your data into a comprehensive risk profile. This isn't about scary predictions—it's about giving you actionable information.
Which Interventions Are Actually Backed by Evidence?
Prevention only works if you act on what you find. Here's what the evidence shows actually moves the needle:
When Medication Is Warranted
- Statins — still the foundation for managing LDL cholesterol and ASCVD risk
- PCSK9 inhibitors — for very high-risk patients or those who can't tolerate statins
- Aspirin — low-dose may be appropriate for some (not all) patients with elevated risk
- Anticoagulation — critical for AFib patients to prevent stroke
- Lp(a)-lowering therapies — new medications are in development; in the meantime, aggressive LDL management helps
Lifestyle: The Foundation
No amount of technology replaces the basics:
- Movement — aim for 7,500–10,000 steps daily plus strength training
- Sleep — 7–9 hours, consistent schedule
- Stress management — chronic stress drives inflammation
- Diet — Mediterranean-style eating pattern, limited processed foods
Supplements (When Appropriate)
Some patients benefit from:
- Omega-3 fatty acids — especially with high triglycerides
- CoQ10 — particularly when on statins
- Vitamin D — if deficient
- Nattokinase — some evidence for cardiovascular support
We personalize recommendations based on your specific results.
What Should You Do Next?
If any of this resonated with you—maybe you have a family history of heart disease, maybe you've had borderline lab results, maybe you just want to know your real risk—here's your action plan:
- Schedule a comprehensive evaluation — We'll run the tests that actually matter, including Lp(a) and CIMT imaging.
- Bring your wearable data — If you have a smartwatch, we want to see it.
- Know your numbers — Not just cholesterol, but the full picture: inflammation, metabolic health, genetic risk.
- Act early — The best time to prevent heart disease is now.
See our membership plans and get started →
The future of cardiology isn't about better surgeries or stronger medications. It's about seeing risk coming and stopping it before it starts.
We'd love to help you understand where you stand. Explore CIMT imaging or view our pricing to take the first step.
References
-
Perez MV, Mahaffey KW, Hedlin H, et al.; Apple Heart Study Investigators. Large-Scale Assessment of a Smartwatch to Identify Atrial Fibrillation. N Engl J Med. 2019;381(20):1909–1917. https://pubmed.ncbi.nlm.nih.gov/31722151/
-
Weng SF, Reps J, Kai J, Garibaldi JM, Qureshi N. Can machine-learning improve cardiovascular risk prediction using routine clinical data? PLoS One. 2017;12(4):e0174944. https://pubmed.ncbi.nlm.nih.gov/28376093/
-
Reyes-Soffer G, Ginsberg HN, Berglund L, et al. Lipoprotein(a): A Genetically Determined, Causal, and Prevalent Risk Factor for Atherosclerotic Cardiovascular Disease: A Scientific Statement From the American Heart Association. Arterioscler Thromb Vasc Biol. 2022;42(1):e48–e60. https://pubmed.ncbi.nlm.nih.gov/34647487/
-
Zhuang B, Sirajuddin A, Zhao S, Lu M. The role of 4D flow MRI for clinical applications in cardiovascular disease: current status and future perspectives. Quant Imaging Med Surg. 2021;11(9):4193–4210. https://pubmed.ncbi.nlm.nih.gov/34476199/
Ready to see your actual risk?
Advanced metabolic testing, arterial imaging, and a personalized prevention plan — built around your numbers.
View Memberships