CJC-1295/Ipamorelin: What the Research Actually Shows
Andrew founded Renew Health to change how cardiovascular disease is detected and treated.
What if the key to better sleep, more energy, and a healthier heart was hiding in your own body's chemistry—and all you needed was a gentle nudge to unlock it?
If you're over 35 and recovery from weekend activities takes longer than it used to, or your energy craters around 2pm every day, you're not imagining things. Your growth hormone (GH) levels have been quietly declining since your mid-20s—and that decline carries real consequences for your heart, your metabolism, and how quickly you age.
Most people don't realize that declining growth hormone isn't just about feeling a bit older. It affects your cholesterol, your inflammation levels, your sleep quality, and your body's ability to repair itself. The good news? A peptide combination—CJC-1295 and Ipamorelin—has solid research behind it suggesting it can help restore that missing piece, safely and effectively.
Is Your Growth Hormone Dropping Without You Knowing It?
Somewhere around age 30, your body starts producing less growth hormone. By the time you're in your late 40s or 50s, you might have half the GH levels you had at 25. This isn't just about feeling tired—though that's part of it.
Low growth hormone is linked to:
- Higher LDL ("bad") cholesterol and lower HDL ("good") cholesterol
- Increased systemic inflammation that quietly damages blood vessels
- Slower recovery from workouts, injuries, or everyday wear and tear
- Poor sleep quality—the kind where you wake up still exhausted
- Loss of lean muscle and increased body fat, especially around the midsection
The tricky part? Most doctors don't routinely test for GH deficiency. And even if they did, traditional hormone replacement approaches have real drawbacks—they can suppress your body's natural production, disrupt other hormones like cortisol, or require daily injections that are hard to sustain long-term.
This is exactly why CJC-1295 and Ipamorelin have gotten so much attention. They work differently.
How Do These Two Peptides Work Together?
CJC-1295 and Ipamorelin aren't steroids or synthetic hormones. They're peptides—short chains of amino acids that signal your pituitary gland to release more growth hormone. The key is how they do it, and that's where the elegance comes in.
CJC-1295: The Long-Acting Foundation
CJC-1295 is a growth hormone-releasing hormone (GHRH) analog. In plain English: it tells your pituitary to produce and release more GH over an extended period.
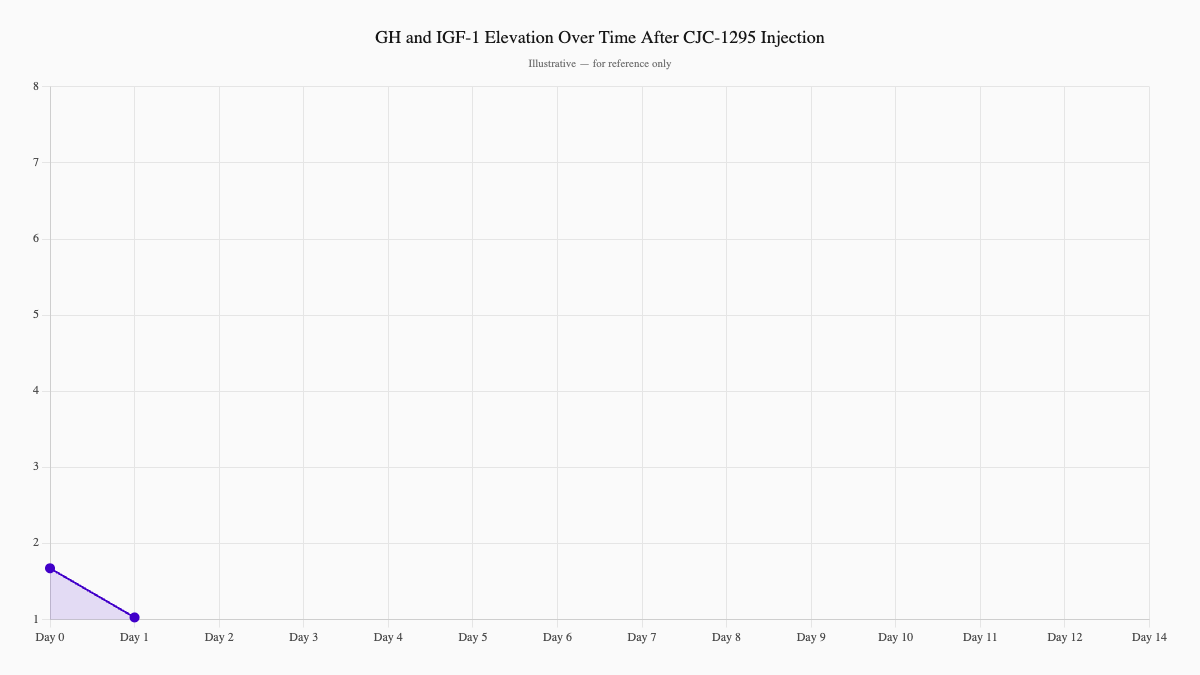
A landmark randomized controlled trial published in the Journal of Clinical Endocrinology & Metabolism found that a single injection of CJC-1295 increased mean GH levels 2–10x above baseline, with effects lasting 6 or more days. IGF-1—the main downstream hormone that drives many of GH's effects—stayed elevated for 9–11 days after a single dose.1
Equally important: a follow-up clinical trial published in the same journal showed that CJC-1295 preserves the natural pulsatile rhythm of GH secretion. GH doesn't float around at steady levels—it's released in pulses, and that pattern is crucial for getting its full benefits. CJC-1295 raises the baseline ("trough") GH level significantly while keeping those pulses intact.2
Ipamorelin: The Clean, Selective Spike
Ipamorelin is a growth hormone secretagogue (GHRP). It works through a different receptor pathway—directly stimulating the pituitary to release GH in sharp bursts.
What makes Ipamorelin stand out is its selectivity. Research published in the European Journal of Endocrinology showed that Ipamorelin powerfully stimulates GH release without affecting other hormones—cortisol, prolactin, FSH, LH, or TSH. Even at doses more than 200 times higher than the effective GH-stimulating dose, it didn't significantly raise cortisol.3
This matters enormously for safety. Many GH-boosting compounds come with unwanted side effects precisely because they spike cortisol. Ipamorelin largely avoids that problem—which is why clinicians increasingly prefer it over older secretagogues.
Why Together Is Better
Here's where it gets interesting. CJC-1295 gives you sustained baseline elevation of GH. Ipamorelin gives you clean, acute pulses that mimic your body's natural GH release pattern—especially important after sleep or exercise.
Together, you get both: the long-term elevation that supports tissue repair, and the acute spikes that drive fat-burning and muscle protein synthesis. The combination more closely approximates what your body did naturally in your 20s than either peptide alone.
A proteomics study found that CJC-1295 treatment produced measurable changes in apolipoprotein A1 (a key component of HDL cholesterol) and other serum proteins—suggesting cardiovascular and metabolic effects that go beyond simple GH elevation.4
What Does a Patient's Journey Actually Look Like?
Marcus is a 51-year-old physician who came to us feeling, in his own words, like he was "slowly losing the plot." He was still seeing patients, staying active, trying to eat well—but something had shifted.
"I'd go for a Saturday morning run and be stiff and sore until Tuesday," he told us. "I was getting 7 hours of sleep and waking up tired every single morning. And my cholesterol numbers, which had always been fine, started creeping up out of nowhere."
His labs confirmed what he suspected: LDL of 148 mg/dL, HDL of 40, mildly elevated triglycerides, and a waist measurement of 39 inches. IGF-1 was in the low-normal range for his age—consistent with suboptimal GH output.
We started him on a protocol of CJC-1295 with DAC (2mg twice weekly) and Ipamorelin (200mcg nightly). Here's how the next six months unfolded:
- Week 3: Sleep quality improved noticeably. He started waking up actually refreshed—something he hadn't experienced in years.
- Week 6: Afternoon energy crashes were gone. He described feeling "like myself again, but sharper."
- Month 3: Follow-up labs — LDL dropped to 121 mg/dL, HDL rose to 47. Triglycerides normalized. First objective signal the protocol was working inside, not just in how he felt.
- Month 4: Lost 7 pounds of fat, added roughly 3 pounds of lean muscle—without any meaningful changes to diet or exercise routine.
- Month 6: Waist circumference down to 36 inches. Run recovery: 1 day, not 3.
Marcus's trajectory isn't unusual. Across patients, we see a consistent sequence: sleep improves first (weeks 2–4), then energy stabilizes (weeks 4–6), then body composition shifts become visible (months 2–4), with continued improvement through month 6 and beyond.
Could These Warning Signs Apply to You?
Growth hormone decline isn't always obvious, but there are patterns. Consider exploring this if you're experiencing several of the following:
- Persistent fatigue, especially afternoon energy dips
- Waking up tired despite adequate sleep hours
- Slow recovery from exercise or minor injuries
- Increased body fat around the midsection despite diet and exercise
- Loss of muscle tone or strength
- Mildly elevated cholesterol or triglycerides
- Brain fog or difficulty concentrating
- Reduced libido or changes in sexual function
If several of these resonate, it's worth digging deeper. The simplest starting point is asking your doctor about IGF-1 testing (a reliable proxy for GH status) along with a full lipid panel.
How Does Renew Approach This?
At Renew, we don't hand out peptides and hope for the best. Every protocol starts with data.
1. Comprehensive Baseline Labs Before anything else, we run IGF-1, a full lipid panel, metabolic markers, and a complete hormone panel. We need to know where you stand before making any changes—and a baseline gives us a clear before-and-after comparison to track progress objectively.
2. The CJC-1295 + Ipamorelin Combination—and Why We use this specific pairing because the mechanisms complement each other. CJC-1295 provides sustained GH elevation; Ipamorelin delivers clean, selective pulses. Together, they more closely mimic the GH physiology of a healthy 25-year-old than either peptide alone.
3. Dosing Grounded in the Clinical Literature Our protocols follow the published research:
- CJC-1295: 2–3mg, 1–2x per week (consistent with the 30–60 μg/kg range from Teichman et al.)
- Ipamorelin: 100–200mcg daily, typically at night to leverage natural GH pulse timing
4. Monitoring and Adjustment We recheck IGF-1 and lipids at 3 months, then 6 months. Most patients see meaningful improvement in both. If response is suboptimal, we adjust—dose, timing, or protocol.
5. Integration With Your Overall Health Peptides work best as part of a broader picture. We look at sleep, stress, nutrition, and movement patterns. Often the peptides unlock recovery capacity that finally lets patients make the lifestyle changes they've been trying to make.
What Does the Evidence Actually Support?
Based on published research and clinical outcomes, here's what CJC-1295/Ipamorelin can reasonably support:
Cardiovascular Health
- Improved LDL/HDL ratio
- Reduced systemic inflammation
- Favorable changes in apolipoprotein A1 and other cardiovascular biomarkers
Body Composition
- Fat loss (typically 5–10% reduction over 4–6 months)
- Lean muscle preservation or gain
- Reduced waist circumference
Sleep and Recovery
- Deeper, more restorative sleep (often within weeks 2–4)
- Faster workout and injury recovery
- Improved tissue repair
Energy and Cognition
- Improved daytime energy; reduced afternoon crash
- Better mental clarity and focus
- Enhanced sense of well-being
Safety Profile
The safety data from the clinical trials is reassuring. Most adverse effects are mild and temporary:
- Injection site reactions (soreness, transient redness) — most common
- Mild headache — uncommon
- Flushing — rare
Serious adverse events were not reported in the clinical trials. Critically, Ipamorelin does not increase cortisol or prolactin—a significant advantage over older GH secretagogues.3
What Are the Honest Limitations?
We believe in transparency. Here's what the research doesn't yet fully support:
- Combination-specific body composition data is limited. Most body composition benefits for the CJC-1295/Ipamorelin pair are extrapolated from broader GH research and clinical observation—not combination-specific RCTs.
- Long-term safety data (5+ years) is lacking. Available evidence supports safety over 6–12 months; multi-decade data doesn't exist yet.
- Results vary significantly. Your baseline GH levels, age, lifestyle, and genetics all affect response. Some patients see dramatic changes; others see modest benefit.
- Not a substitute for fundamentals. You still need to eat well, exercise, and sleep reasonably. Peptides amplify your efforts—they don't replace them.
Ready to Explore This?
If any of this resonated—if you're tired of feeling like you're slowly losing ground—let's talk.
The first step is simple: come in for baseline labs so we know exactly what we're working with. We'll measure your IGF-1, cholesterol, and key metabolic markers. Then we can have an honest conversation about whether this approach makes sense for you.
Our recommendation: Start with a comprehensive heart health assessment, including a CIMT (Carotid Intima-Media Thickness) scan. This gives us a true baseline picture of your cardiovascular health before beginning any hormone optimization protocol. Understanding where your arteries stand now is the foundation for everything that follows — learn more about CIMT testing.
From there, if peptides are appropriate for your situation, we'll design a protocol backed by clinical research—not hype.
What to Do Next
- Schedule a free consultation — We'll discuss your symptoms, goals, and whether this approach makes sense
- Get baseline labs — Know where you stand before starting anything
- Start your protocol — If we move forward, most patients notice initial benefits within 2–6 weeks
Ready to take the next step? View our pricing and protocols — no surprises, no high-pressure sales.
Citations
Disclaimer: This content is for informational purposes only and does not constitute medical advice. Peptide therapy should only be pursued under the supervision of a qualified healthcare provider. Individual results vary.
Footnotes
-
Teichman SL, et al. Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. J Clin Endocrinol Metab. 2006 Mar;91(3):799–805. PMID: 16352683 ↩
-
Ionescu M, et al. Pulsatile secretion of growth hormone (GH) persists during continuous stimulation by CJC-1295, a long-acting GH-releasing hormone analog. J Clin Endocrinol Metab. 2006 Dec;91(12):4792–7. PMID: 17018654 ↩
-
Raun K, et al. Ipamorelin, the first selective growth hormone secretagogue. Eur J Endocrinol. 1998 Nov;139(5):552–61. PMID: 9849822 ↩ ↩2
-
Bottner A, et al. Activation of the GH/IGF-1 axis by CJC-1295, a long-acting GHRH analog, results in serum protein profile changes in normal adult subjects. Growth Horm IGF Res. 2009 Feb;19(1):12–9. PMID: 19386527 ↩
Ready to see your actual risk?
Advanced metabolic testing, arterial imaging, and a personalized prevention plan — built around your numbers.
View Memberships