The Cardiology Problem Nobody's Talking About: How Poor Sleep Damages Your Arteries
Andrew founded Renew Health to change how cardiovascular disease is detected and treated.
Most people know sleep matters. Very few know just how directly it's reshaping their heart.
Not in a vague "rest is good for you" way. In a measurable, visible, you-can-see-it-on-an-ultrasound way. Research now shows that chronic short sleep — fewer than six hours a night — is associated with a 48% higher risk of coronary heart disease. And the damage doesn't wait until you feel tired. It's accumulating in your arterial walls right now, years before any symptoms appear.
Sleep is, in a very real sense, cardiovascular medicine. And most people — and most doctors — aren't treating it that way.
Why Does Standard Care Miss the Sleep-Heart Connection?
Your annual checkup probably includes cholesterol, blood pressure, and maybe blood sugar. What it almost certainly doesn't include is a real assessment of your sleep.
That's a problem.
Sleep is when your cardiovascular system does its repair work. Your heart rate drops. Blood pressure falls. Stress hormones recede. Inflammatory cytokines get cleared. Your body patches the microscopic damage that accumulates throughout the day in your blood vessels.
When sleep is consistently cut short — or when it's fragmented by undiagnosed sleep apnea — none of that repair happens properly. Night after night, the damage goes unaddressed. And over years, it adds up.
Conventional medicine treats sleep as a lifestyle variable, not a cardiovascular risk factor. That's why millions of people are walking around with sleep apnea they don't know about, inflammation they can't feel, and arterial walls quietly thickening in the background.
What Happens to Your Arteries When You Don't Sleep?
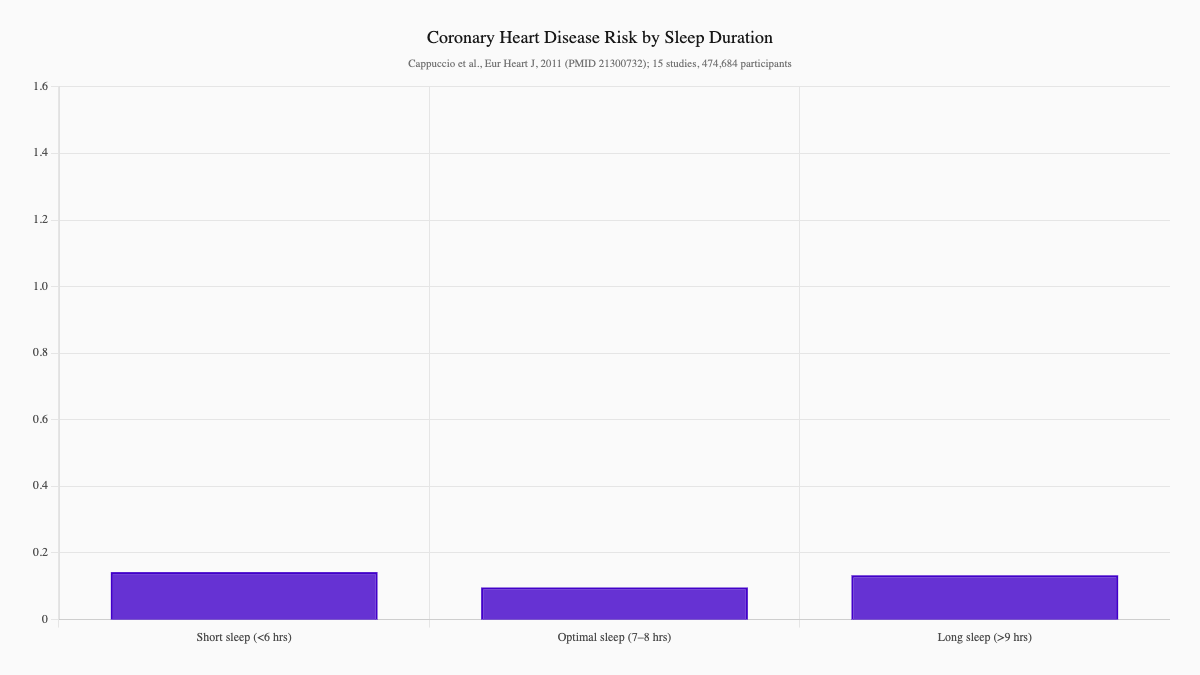
Sleep Duration and Coronary Heart Disease Risk
A landmark systematic review and meta-analysis published in the European Heart Journal analyzed 15 prospective studies covering 474,684 participants followed for up to 25 years. The findings were striking: short sleep duration (typically defined as fewer than six hours) was associated with a 48% greater risk of coronary heart disease and a 15% greater risk of stroke. Long sleep duration — more than nine hours — also raised risk, suggesting that optimal cardiovascular health sits in a narrower window than most people realize: seven to eight hours per night. (Cappuccio et al., 2011, European Heart Journal, PMID: 21300732)
Sleep Deprivation and Cardiovascular Disease Risk
A more recent systematic meta-analysis pooled 18 cohort studies of adult populations and found that sleep deprivation (≤5 or ≤6 hours per night) was independently associated with a 9% higher risk of cardiovascular disease (RR: 1.09, 95% CI: 1.02–1.16). That may seem modest in isolation — but compounded over years, and layered on top of other risk factors like insulin resistance or hypertension, the effect is clinically significant. (Pan et al., 2023, Biomedical Reports, PMID: 37829258)
Sleep Apnea, Short Sleep, and Arterial Wall Thickening
One of the most compelling findings in sleep-cardiovascular research comes from the ELSA-Brasil study, a large longitudinal cohort that examined the link between obstructive sleep apnea (OSA), sleep duration, and carotid intima-media thickness (CIMT) — the gold-standard measure of subclinical atherosclerosis. The study found that both OSA severity and short sleep duration were independently associated with increased CIMT, even after adjusting for traditional cardiovascular risk factors. This means sleep wasn't just a marker — it was doing something to the artery walls themselves. (Souza et al., 2021, Arteriosclerosis, Thrombosis, and Vascular Biology, PMID: 33567870)
Poor Sleep Quality and Subclinical Atherosclerosis
It's not only about how long you sleep — quality matters too. A 2023 study in Frontiers in Epidemiology assessed sleep quality (using the validated Pittsburgh Sleep Quality Index) and carotid IMT in 110 otherwise healthy young adults. Despite having no known cardiovascular disease, 44.5% already showed increased CIMT. Poor sleep quality — particularly prolonged sleep onset latency and reduced sleep efficiency — was independently associated with greater arterial wall thickness. (Sethi et al., 2023, Frontiers in Epidemiology, PMID: 38455319)
How Does Sleep Deprivation Damage the Heart?
Understanding why sleep affects cardiovascular health helps clarify why this is so much more serious than "feeling tired."
1. Cortisol dysregulation. Poor sleep chronically elevates cortisol — the primary stress hormone. High cortisol accelerates arterial inflammation, promotes insulin resistance, and raises blood pressure. What starts as "I'm not sleeping great" becomes a sustained physiological stress response.
2. Sympathetic nervous system overdrive. During normal sleep, the sympathetic (fight-or-flight) nervous system quiets down. Without adequate sleep, it stays elevated — keeping heart rate and blood pressure elevated even at rest.
3. Inflammatory cytokine surge. Sleep deprivation raises levels of IL-6, TNF-alpha, and other pro-inflammatory proteins. These are the same molecules that destabilize atherosclerotic plaque and accelerate its growth.
4. Impaired endothelial function. The inner lining of your arteries — the endothelium — requires overnight recovery time. Poor sleep impairs nitric oxide production, which the endothelium uses to stay flexible and responsive. Without it, arteries stiffen.
5. Blood pressure that never fully drops. In healthy sleepers, blood pressure dips 10–20% overnight (called "dipping"). Non-dippers — whose pressure stays elevated through the night — have dramatically higher rates of heart attack and stroke. Fragmented or insufficient sleep prevents this dip from occurring.
What Are the Warning Signs Most People Ignore?
Sleep disorders and sleep deprivation often go unrecognized because the symptoms are easy to rationalize. Watch for:
Classic signs of poor sleep quality:
- Difficulty falling asleep or staying asleep
- Waking unrefreshed despite a full night
- Daytime fatigue, brain fog, or difficulty concentrating
- Irritability or mood instability
- Relying on caffeine to function through the afternoon
Signs that may indicate sleep apnea:
- Loud snoring
- Waking with headaches or a dry mouth
- Gasping or choking during sleep (often reported by a partner)
- Frequent nighttime urination
- High blood pressure that's difficult to control
- Waking unrefreshed even after 8+ hours
Many people with sleep apnea have none of the "classic" signs. They don't snore loudly, they're not overweight, and they don't feel obviously sleepy during the day. The only way to know for certain is a sleep study.
James's Story: What Did a Preventive Evaluation Uncover?
James was 52 when he came to Renew for a preventive cardiovascular evaluation. He was fit — he ran three times a week — and his cholesterol panel looked fine. But he'd been waking up tired for years. He assumed it was stress. His primary care doctor hadn't flagged anything.
His CIMT scan told a different story. For his age, his carotid arterial wall thickness was in the 75th percentile — thicker than three-quarters of men his age. His blood pressure wasn't well-controlled overnight (confirmed by 24-hour ambulatory monitoring). He had elevated hs-CRP and mildly elevated fasting insulin.
We referred him for a home sleep study. The results: moderate obstructive sleep apnea, with an apnea-hypopnea index of 22 events per hour. James had been quietly suffocating dozens of times each night for years, with no one catching it.
After six months on CPAP therapy, combined with dietary changes to address insulin resistance, his morning blood pressure normalized, his hs-CRP dropped from 2.8 to 1.1 mg/L, and his energy returned. His follow-up CIMT showed no progression. We caught it just in time to reverse course.
How Does Renew Treat Sleep as a Cardiovascular Intervention?
At Renew, we evaluate sleep as a core component of cardiovascular health — not an afterthought.
Our sleep-cardiovascular assessment includes:
-
CIMT imaging — Direct visualization of carotid arterial wall thickness and plaque. If sleep disorders are contributing to vascular damage, we often see it here first. Learn more about our CIMT testing →
-
24-hour ambulatory blood pressure monitoring — To detect nocturnal non-dipping, which is often linked to sleep apnea and dramatically elevates cardiovascular risk.
-
Inflammatory biomarker panel — hs-CRP, Lp-PLA2, and other markers that reflect the inflammatory burden that poor sleep generates.
-
Metabolic assessment — Fasting insulin, HbA1c, and triglyceride/HDL ratio. Sleep deprivation promotes insulin resistance, which compounds cardiovascular risk.
-
Sleep apnea screening — We use validated tools (Berlin Questionnaire, Epworth Sleepiness Scale) to assess risk, and refer for home or in-lab sleep studies when indicated.
-
Comprehensive cardiovascular risk review — Integrating all findings into a personalized picture of where your risk actually stands.
What Works for Sleep Optimization? Evidence-Based Strategies for Heart Health
If your sleep is poor — or if you haven't been evaluated — here's what to do:
First priority: Rule out sleep apnea. If you snore, wake unrefreshed, have resistant hypertension, or have a thick neck circumference, ask for a sleep study. CPAP therapy for moderate-to-severe OSA reduces blood pressure, lowers inflammatory markers, and stabilizes arterial function. Don't skip this step.
Sleep hygiene (foundational, always start here):
- Consistent sleep and wake times — even on weekends
- Cool, dark, quiet sleeping environment (blackout curtains, white noise if needed)
- No screens 60 minutes before bed (blue light suppresses melatonin)
- No alcohol within 3 hours of sleep (it fragments sleep architecture even if it helps you fall asleep initially)
- Cut caffeine off by 1–2 PM
Address the underlying physiology:
- Magnesium glycinate (300–400 mg nightly) — commonly depleted; supports nervous system relaxation and sleep quality
- Optimize vitamin D — low vitamin D is linked to sleep disorders; target 50–80 ng/mL
- Manage cortisol — chronic stress is a major sleep disruptor; addressing it directly (therapy, meditation, adaptogenic support) has meaningful downstream cardiovascular effects
Treat insulin resistance — elevated blood glucose disrupts sleep architecture. Fixing metabolic health often dramatically improves sleep.
Physical activity — Regular moderate exercise (150+ minutes per week) reliably improves sleep quality and reduces sleep apnea severity in overweight individuals.
What Should You Do Next?
If you're over 40 — or if you have any cardiovascular risk factors — sleep deserves to be part of your evaluation.
Here's where to start:
-
Track your sleep for one week. Note when you go to bed, when you wake, whether you feel rested, and how much caffeine you're relying on. Patterns reveal more than single data points.
-
Ask your doctor about sleep apnea screening — especially if you snore, have hypertension, or wake unrefreshed.
-
Get your arteries evaluated. A CIMT scan gives you a direct measure of subclinical atherosclerosis that no blood test can provide. If your arteries are already showing age-related changes, you need to know — and act — now.
Ready to See What's Really Going On in Your Arteries?
Sleep, inflammation, arterial health — these systems are deeply connected. At Renew, we look at all of them together, because that's the only way to get a complete picture of your cardiovascular risk.
Our comprehensive evaluation includes a CIMT ultrasound, advanced inflammatory and metabolic biomarkers, sleep apnea screening, and a personalized treatment plan built around your actual physiology — not population averages.
See our evaluation packages and pricing →
The best time to find a problem is before it becomes a crisis. Let's look together.
References
-
Cappuccio FP, et al. Sleep duration predicts cardiovascular outcomes: a systematic review and meta-analysis of prospective studies. European Heart Journal. 2011;32(12):1484–92. PMID: 21300732
-
Pan Y, et al. The association between sleep deprivation and the risk of cardiovascular diseases: A systematic meta-analysis. Biomedical Reports. 2023. PMID: 37829258
-
Souza SP, Santos RB, et al. Obstructive Sleep Apnea, Sleep Duration, and Associated Mediators With Carotid Intima-Media Thickness: The ELSA-Brasil Study. Arteriosclerosis, Thrombosis, and Vascular Biology. 2021;41(4):1549–1557. PMID: 33567870
-
Sethi PP, et al. Poor quality sleep is associated with greater carotid intima media thickness among otherwise healthy resident doctors. Frontiers in Epidemiology. 2023;2:1044111. PMID: 38455319
This article is for educational purposes and does not constitute medical advice. Always consult with a qualified healthcare provider before making changes to your health regimen.
Ready to see your actual risk?
Advanced metabolic testing, arterial imaging, and a personalized prevention plan — built around your numbers.
View Memberships